Climbing a flight of stairs shouldn't feel like a major event. But if you've ever stopped halfway to catch your breath, or felt oddly wiped out after carrying groceries, you already know something important. Breathing isn't just about your lungs. It shapes your energy, your pace, your recovery, and how confident you feel moving through the day.
A lot of people assume breathlessness means they're out of shape. Sometimes that's part of it. But often, the underlying cause starts much deeper in the lungs, inside tiny air sacs called alveoli. They're so small you'll never feel them working, yet every step, stretch, and lift depends on them doing their job well.
That matters whether you're recovering from surgery, trying to get back to exercise, managing pain, or noticing that posture changes your breathing more than you expected. Even something as routine as how you sit during the workday can affect how easily your chest expands and how efficiently you breathe. If that sounds familiar, this guide on how to improve posture while sitting at a desk can help connect body position with breathing comfort.
Introduction Why Your Breath Is Your Power
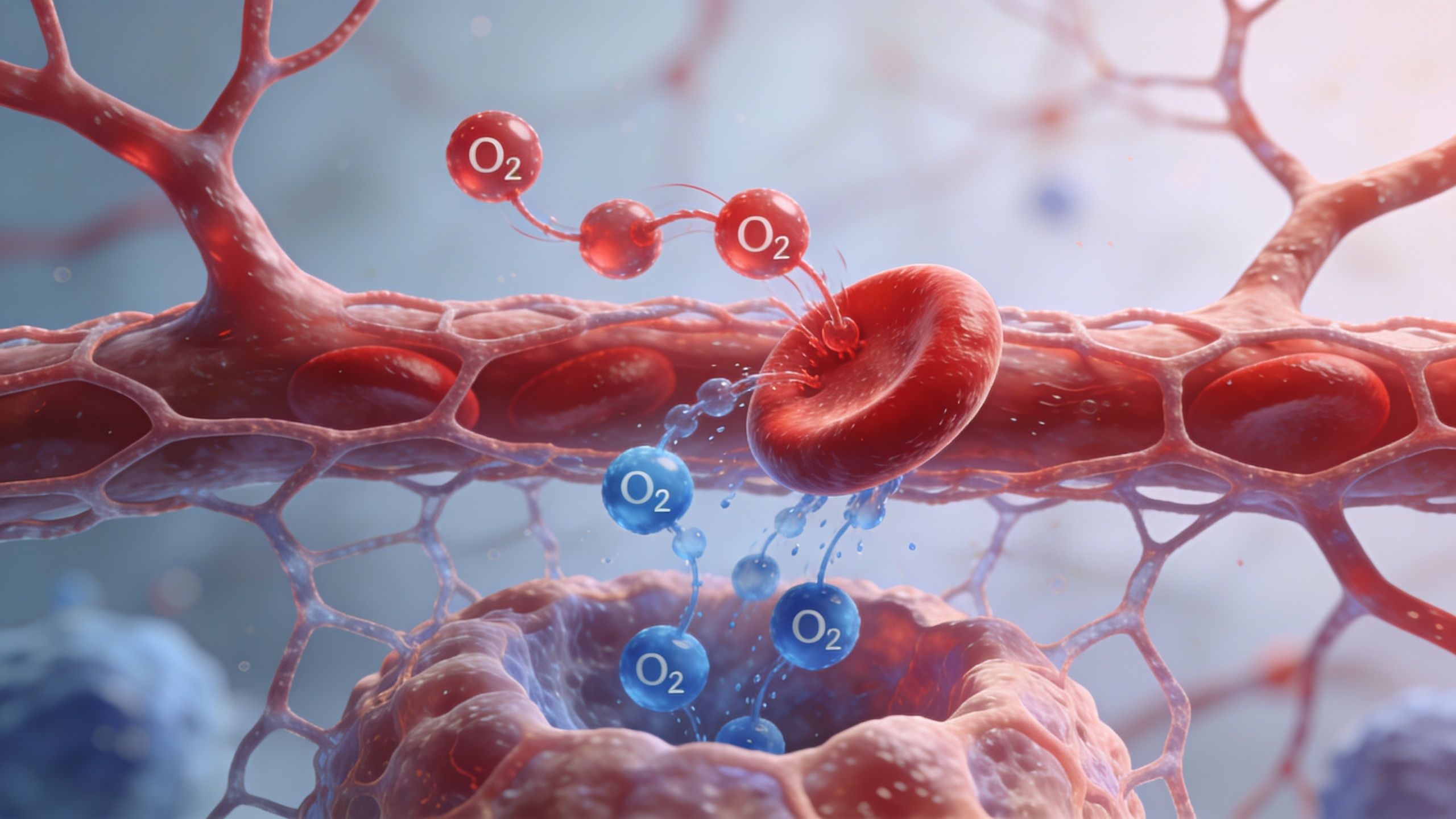
When you inhale, air travels down a branching system of tubes until it reaches the far edges of the lungs. At the end of that journey are the alveoli. They're the true work sites of breathing. Oxygen moves into your blood there, and carbon dioxide moves out.
That exchange sounds simple. It isn't. Your body has to do it constantly, unobtrusively, and fast enough to keep up whether you're sleeping, walking, or climbing stairs with laundry in your arms.
Breathing well isn't only about feeling calm. It's about giving your muscles the oxygen they need to move without burning out too soon.
If the alveoli are healthy, your body has a better supply line. Muscles work more efficiently. Your heart doesn't have to strain as much to deliver oxygen. Activity feels smoother and less threatening.
If the alveoli are irritated, collapsed, filled with fluid, or damaged, the whole body feels it. You may notice shortness of breath, slower recovery after activity, fatigue that seems out of proportion, or that heavy-chested feeling that makes movement feel harder than it should.
Why patients get confused
Many people think breathing trouble should always feel dramatic. Often it doesn't. Sometimes it shows up as:
- Early fatigue: You tire out faster than expected during chores or exercise.
- Needing more breaks: You pause during activity, not because of pain alone, but because your breathing won't settle.
- Reduced confidence: You move less because breathlessness feels uncomfortable or unpredictable.
The good news is that once you understand alveoli, a lot of these symptoms start to make sense. And when symptoms make sense, rehab feels less mysterious.
The Architecture of Your Lungs' Tiniest Workers
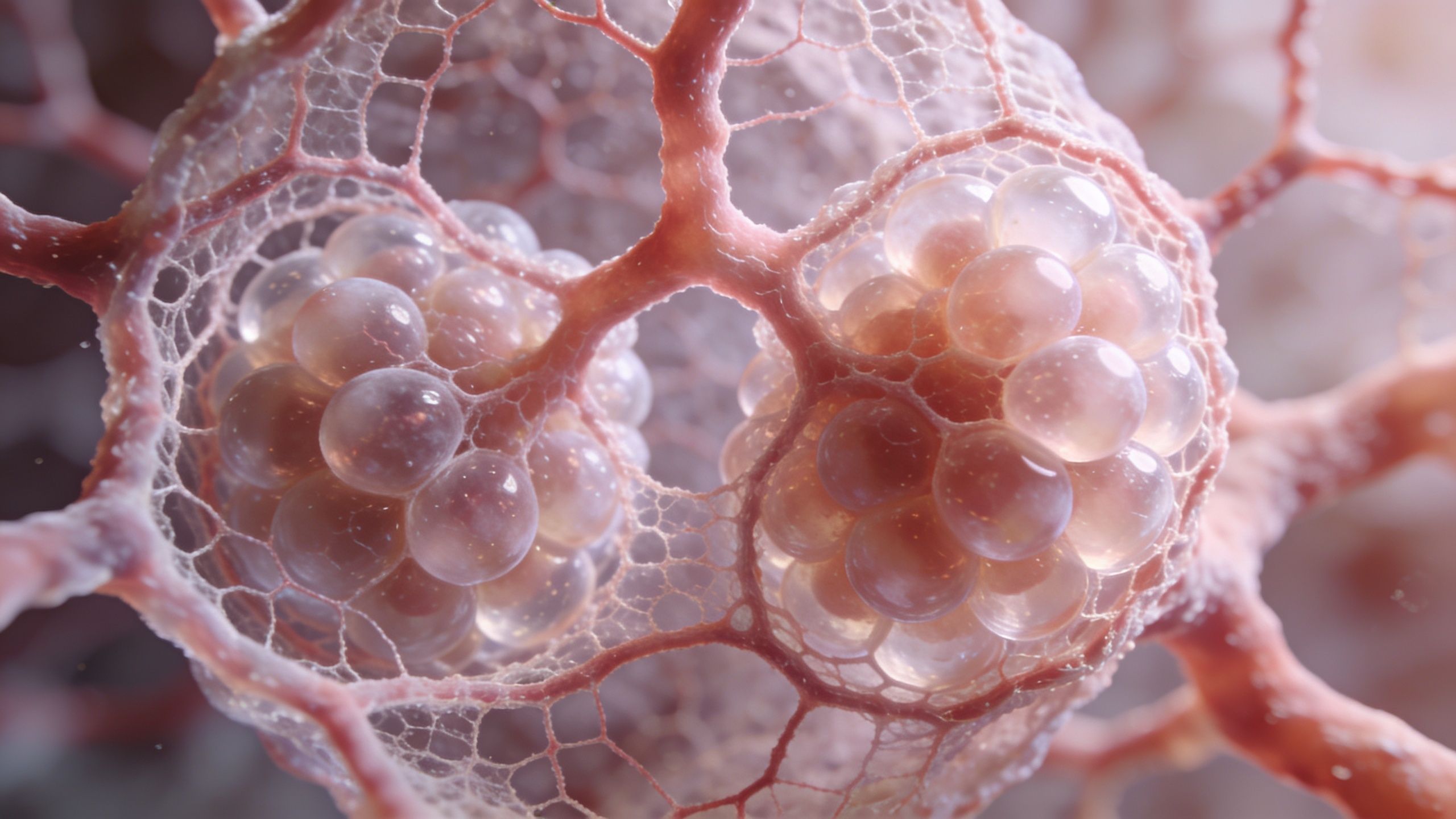
The easiest way to picture alveoli is to think of a cluster of grapes at the end of very small airways. Each grape-like sac is a place where air meets blood. That's where the body loads oxygen in and unloads carbon dioxide out.
The scale is hard to grasp until you attach numbers to it. Human lungs contain an average of 480 million alveoli, creating 70 to 80 square meters of surface area, roughly the size of a tennis court, according to Kenhub's alveoli anatomy overview. That huge surface is how your lungs manage to exchange gases efficiently without taking up your whole body.
Built for contact
Alveoli work because their walls are extremely thin and they sit right next to a dense capillary network. Oxygen doesn't have to travel far. It crosses from air to blood across a microscopic barrier designed for speed.
Kenhub notes that Type I cells cover 95% of this surface, and the air-blood barrier is just 0.1 to 1 micrometer thick in the alveoli's gas exchange region. That thinness is one reason healthy lungs can respond so quickly when your body suddenly needs more oxygen.
Here's a simple way to understand it:
- Air arrives: You inhale and bring oxygen into the alveoli.
- Blood passes by: Tiny capillaries wrap around the sacs.
- Exchange happens: Oxygen moves into blood, and carbon dioxide moves out to be exhaled.
Two cell types, two key jobs
The alveoli aren't just empty balloons. They're lined by specialized cells with different jobs.
- Type I cells: These form most of the exchange surface. They're thin and flat, which helps gases move across quickly.
- Type II cells: These produce surfactant, a slippery substance that helps keep the alveoli open.
Patients often get stuck on the word “cells” and assume this is too microscopic to matter in real life. It matters a lot. If the exchange surface gets damaged, or if the lining stops supporting the sacs properly, you don't just lose a biology fact. You lose breathing efficiency.
Practical rule: Tiny structures can create huge symptoms. When enough alveoli stop working well, even light activity can feel harder.
Why so many alveoli matter
Your body doesn't rely on one large chamber for gas exchange. It relies on millions of tiny sacs spreading the work out over an enormous surface. That design gives you reserve capacity. It helps you meet changing demands from rest to exercise.
It also means that when disease affects the alveoli, the problem may be widespread even if you can't see it from the outside. A person may look fine sitting still, then become winded the moment movement raises oxygen demand.
How the Miracle of Gas Exchange Actually Works
Every breath sets up a transfer. Air enters the alveoli. Blood flows through nearby capillaries. Oxygen moves one way, carbon dioxide moves the other way. It happens automatically, but it depends on delicate mechanics staying intact.
If you want a simple analogy, think of the alveoli as tiny soap bubbles that must stay open, flexible, and connected to blood flow. If they stiffen, collapse, or fill up, gas exchange becomes less efficient.
Why alveoli don't collapse with every exhale
One of the biggest points of confusion is this: if alveoli are so small, why don't they just snap shut all the time?
Part of the answer is surfactant. The alveolar lining contains this substance, which acts a bit like a non-stick coating. It lowers surface tension so the sacs can stay open more easily during exhalation. According to Deranged Physiology's review of alveolar structure and function, surfactant reduces surface tension and increases pulmonary compliance by up to 10-fold, helping prevent alveolar collapse.
The walls also contain structural fibers with different jobs:
- Elastic fibers: These give alveoli stretch and recoil.
- Collagen fibers: These add support and help resist over-distension.
Why exhalation can feel easy or hard
Healthy lungs don't just inflate. They also spring back. That recoil helps push air out without you having to force every exhale.
When elastic fibers are working well, exhalation is more efficient. When that system is damaged, air can get trapped, breathing becomes more labor-intensive, and people may feel like they can't fully empty their lungs.
That's why some patients say, “I can get air in, but I can't get it out well.” They're often describing a mechanical problem, not a lack of effort.
The work of breathing rises quickly when alveoli lose their spring and stability.
A delicate balance
Gas exchange depends on several things happening at once:
- Air has to reach the alveoli.
- The alveoli have to stay open.
- Blood has to flow past them.
- The barrier between air and blood must stay thin enough for transfer.
If even one part breaks down, the body compensates. You breathe faster. Neck and shoulder muscles jump in. Activity becomes more tiring. That's often where patients first notice something is wrong.
When Your Alveoli Are Under Attack
A lot of patients notice the problem during ordinary life first. You walk to the bathroom, climb a few steps, or carry groceries, and your breathing feels out of proportion to the task. That often means the alveoli are being harmed in a specific way, and the pattern of damage changes what movement feels like and what recovery will require.
Alveoli do not all fail the same way. Some lose their walls. Some fill with fluid. Some collapse because the lining that helps hold them open stops working well. For a respiratory therapist or physical therapist, those differences matter because the right breathing strategy for one problem may be the wrong fit for another.
Emphysema in COPD
In emphysema, the tiny walls between neighboring air sacs break down over time. Instead of many small exchange units, the lung develops larger, less efficient spaces. The chest may still feel full of air, but less of that air is reaching a healthy exchange surface.
That helps explain a common patient complaint: “I breathe in, but I still feel short of breath.” The problem is not only airflow. It is also lost working surface inside the lungs. The National Heart, Lung, and Blood Institute describes emphysema as damage to the walls between air sacs that can reduce oxygen transfer and trap air in the lungs, which makes breathing harder during activity (NHLBI overview of COPD).
For daily life, that often means slower walking, longer recovery after exertion, and a feeling that exhalation takes too much effort.
Pneumonia
Pneumonia attacks alveoli differently. The air sacs are still there, but they can fill with fluid, pus, and inflammatory cells. A simple picture is a sponge whose pores are partly waterlogged. Air cannot use that space well.
That is why pneumonia often causes heavy breathing, coughing, chest discomfort, and fast fatigue. A short trip across the room can feel like a workout because the lung is trying to exchange gases through partially blocked air sacs. The American Lung Association explains that pneumonia causes the air sacs in one or both lungs to become inflamed and fill with fluid or pus (American Lung Association on pneumonia).
Indoor air irritation can add to the burden for people who already have sensitive lungs. If you are trying to reduce triggers at home, this guide to protecting families from contaminated air ducts offers a useful overview of why cleaner indoor air may support respiratory comfort.
ARDS
ARDS, or Acute Respiratory Distress Syndrome, is a medical emergency. In ARDS, inflammation spreads across the lungs, fluid leaks into the alveoli, and many air sacs become difficult to keep open. The National Heart, Lung, and Blood Institute notes that ARDS causes fluid buildup in the alveoli, which keeps the lungs from filling with enough air and lowers the amount of oxygen reaching the bloodstream (NHLBI page on ARDS).
When many alveoli are unstable at once, oxygen levels can fall quickly. People with ARDS often need intensive support because breathing harder alone cannot solve the problem.
Common Conditions Affecting Alveoli
| Condition | Primary Mechanism of Damage | Key Impact on Gas Exchange |
|---|---|---|
| Emphysema | Breakdown of alveolar walls | Less working surface for oxygen and carbon dioxide transfer |
| Pneumonia | Fluid and inflammatory material fill alveoli | Air cannot reach the exchange surface effectively |
| ARDS | Widespread inflammation and fluid-filled, unstable alveoli | Many air sacs stop contributing to oxygen transfer |
Why this distinction matters in rehab
Two people can report the same symptom and need different care. One may need pacing and prolonged exhalation training because air gets trapped. Another may need positioning, gentle mobility, and breathing practice that helps recruit fluid-affected lung regions. A third may be recovering from a critical illness and need a carefully graded return to upright activity because oxygen levels fall with small efforts.
That is where physical therapy becomes practical, not abstract. Once you know how the alveoli are being attacked, you can match breathing work, posture, walking, and exercise to the actual problem. That improves efficiency, lowers unnecessary breathlessness, and helps people get more out of the energy they have during recovery.
How Alveolar Damage Affects Your Whole Body
When alveoli struggle, your body doesn't experience it as a “lung-only” issue. You feel it everywhere. The chain reaction starts with poor gas exchange, but it shows up as fatigue, weakness, reduced endurance, and slower recovery after effort.
Your muscles depend on oxygen to do work. If oxygen delivery becomes less efficient, ordinary activities cost more. Walking across a parking lot may feel like a workout. Climbing stairs may leave your legs heavy and your chest tight. You may start avoiding movement, not because you're lazy, but because your body is protecting itself from a system that feels overloaded.
Why fatigue feels so disproportionate
Patients often say, “I'm barely doing anything. Why am I this tired?” The reason is that when alveoli aren't doing their part, the body has to compensate.
Common compensation patterns include:
- Faster breathing: You try to pull in more air to make up for poor exchange.
- Accessory muscle use: Neck, chest, and shoulder muscles start helping with breathing.
- Higher effort during activity: The same task now takes more energy.
That added work can make you feel drained before your muscles are “worked out” in the usual sense.
If breathing becomes inefficient, movement becomes expensive.
Why movement can decline fast
Once breathlessness leads to less activity, deconditioning often follows. Then the body gets less efficient overall, and the same activity feels even harder next time. Pain can also worsen this cycle. A person with back pain or post-surgical stiffness may already be moving cautiously. Add poor breathing efficiency, and the drop in stamina becomes even more noticeable.
That's why it helps to understand that shortness of breath during activity isn't always a sign of poor motivation. Sometimes it's your body telling you the oxygen delivery system is under strain.
Breathing Strategies to Support Your Lungs
Breathing exercises can seem too simple to matter. They matter when they change mechanics. The goal isn't to “take big breaths” at random. The goal is to help air move more effectively, reduce unnecessary effort, and support better ventilation of the lungs.

One useful concept here is collateral ventilation. Pores of Kohn allow communication between adjacent alveoli, and breathing techniques such as pursed-lip breathing can help optimize that mechanism when some airways are compromised, which is especially relevant in COPD and post-surgical recovery, as discussed in this video on alveolar pores and collateral ventilation.
Diaphragmatic breathing
This is often called belly breathing, but the goal isn't to force your stomach outward. The goal is to let the diaphragm do more of the work and reduce overuse of the upper chest and neck.
Try it this way:
- Set up comfortably: Sit supported or lie on your back with knees bent.
- Place your hands: One on your upper chest, one on your abdomen.
- Inhale gently through your nose: Let the lower hand rise more than the upper one.
- Exhale slowly: Keep the shoulders relaxed.
This can help direct airflow toward the lower parts of the lungs, where breathing is often more efficient. It also tends to calm breathing rate and reduce tension in accessory muscles.
If your chest and rib cage feel stiff, mobility work can help breathing mechanics too. A dynamic chest stretch is one example that may improve how easily the front of the chest opens during inhalation.
Pursed-lip breathing
This is one of the most practical tools for people who feel air-trapped or breathless with exertion.
Use it like this:
- Inhale through your nose
- Exhale through gently pursed lips, as if you're cooling hot soup
- Make the exhale longer and calmer than the inhale
Why it helps: that slight resistance can create back-pressure in the airways, helping them stay open longer during exhalation. That gives trapped air a better chance to escape and may improve how air redistributes through the lungs.
“Smaller, slower breaths often work better than forceful deep breaths when you're short of breath.”
Don't ignore how air enters
These strategies work best when paired with good airway habits. If you're curious about how the route of breathing affects comfort and airway function, this article on comparing mouth breathing and nasal health gives helpful context.
When to use these techniques
Breathing exercises are especially useful:
- Before activity: To settle your pattern and reduce chest tension
- During activity: To control breathlessness while walking or climbing stairs
- After activity: To recover more smoothly
The key is consistency. Breathing retraining works best when you practice before you desperately need it.
How Physical Therapy Restores Breath and Movement
When alveoli are compromised, treatment can't stop at the lungs. The whole body adapts to breathing trouble. That's where physical therapy becomes valuable.
A physical therapist looks at how you breathe, move, pace effort, and recover. That includes posture, rib cage motion, walking tolerance, strength, and how symptoms change during activity. Some people need breathing retraining. Others need graded exercise to improve how efficiently the body uses oxygen. Many need both.
Physical therapy also helps break the cycle of breathlessness leading to inactivity, then inactivity making breathlessness worse. Instead of avoiding movement, you learn how to dose it. That might mean interval walking, positioning strategies, chest mobility work, or strengthening that supports more efficient movement with less strain.
Hands-on care can also play a role in some cases by improving comfort and motion in the chest wall, spine, and surrounding muscles. If you want a clearer picture of that approach, this overview of what manual therapy is in physical therapy explains how clinicians use it alongside exercise and education.
The big idea is simple. Damage to alveoli may start in microscopic air sacs, but recovery happens at the whole-person level. Better breathing supports better movement. Better movement supports better endurance. And that can change daily life in a very real way.
Frequently Asked Questions About Alveoli
Can damaged alveoli heal or regrow?
It depends on the type of damage. Some problems, such as temporary inflammation or fluid in the alveoli, can improve when the underlying condition gets treated. Structural destruction is harder. If alveolar walls are permanently lost, the body may not fully restore the original architecture. Even then, people can often improve function through medical care, breathing strategies, exercise, and rehab.
Is smoking-related alveolar damage permanent?
Some smoking-related changes may persist, especially when the alveolar walls have been destroyed. But quitting still matters. Stopping exposure can reduce ongoing injury and give the rest of the respiratory system a better chance to function as well as possible.
How can I tell if shortness of breath is from my lungs or just being out of shape?
They can overlap. Lung-related breathlessness often feels out of proportion to the task, may come with chest tightness or prolonged recovery, and may not improve just by “pushing through.” Deconditioning can also cause breathlessness, but it usually improves more predictably with gradual training. If you're unsure, a clinician should assess it rather than guess.
Can breathing exercises really make a difference?
Yes, when they're matched to the problem. Breathing exercises can improve mechanics, reduce air trapping, lower unnecessary muscle tension, and help you recover faster during activity. They aren't a cure for every lung problem, but they can make breathing more efficient and movement more manageable.
Why do I feel breathless when my oxygen numbers seem okay?
Breathlessness isn't caused by one factor alone. You can feel short of breath because of airflow limitation, chest wall stiffness, anxiety, poor breathing pattern, deconditioning, or the extra work required to move air. That's why symptoms deserve a full evaluation, not a single-number explanation.
If breathing problems are making movement harder, Highbar Physical Therapy can help you rebuild confidence, improve breathing mechanics, and return to daily activity with a plan that fits your body and goals. A physical therapist can assess how your breathing affects strength, endurance, posture, and recovery, then guide you with targeted treatment that helps you feel better, move freely, and live fully.
