That sharp, deep ache in the back of your shoulder often shows up in a very specific moment. A pitcher feels it when the arm winds back. A swimmer notices it during recovery overhead. An office worker gets the same pain reaching into the back seat or pulling on a jacket. The movement changes, but the complaint sounds similar. “It hurts deep in the back of the joint.”
That pattern often points to shoulder posterior impingement. It’s a form of shoulder impingement where tissues at the back of the joint get compressed during certain positions, especially when the arm moves into abduction and external rotation. Shoulder impingement as a broader category is the leading cause of shoulder pain seen in outpatient clinics, accounting for 44% to 65% of all shoulder complaints, according to the NCBI overview of shoulder impingement syndrome.
If you’re worried that this means something is torn beyond repair, slow down. Posterior impingement can be painful and stubborn, but it’s also a condition physical therapists deal with regularly. The key is getting the mechanism right. A lot of people are told they “just have shoulder pain,” when the underlying issue is how the ball, socket, rotator cuff, and shoulder blade are interacting at the back of the joint.
Introduction What Is That Deep Pain in My Shoulder
The shoulder is built for freedom, not stability, much like a golf ball sitting on a tee. That design lets you reach, throw, swim, lift, and rotate in a huge range. It also means small movement problems can create very specific pain patterns.
With shoulder posterior impingement, the painful pinch happens at the back of the shoulder joint, not the top. That matters. Many people hear “impingement” and assume the problem is always under the acromion near the front or side of the shoulder. Posterior impingement is different. The pain usually shows up when the arm moves up and back, especially in positions that combine abduction and external rotation.
Why this diagnosis gets missed
Athletes get most of the attention in discussions about posterior impingement, and for good reason. It’s common in overhead sports. But active adults who don’t play a throwing sport can still develop the same problem pattern from repeated reaching, poor scapular control, stiffness, or work demands.
A deep pain at the back of the shoulder during a very particular movement is not “all in your head” and it isn’t automatically a random strain.
What helps most is understanding two things:
- Where the pain is coming from: the back of the joint, where the posterior rotator cuff and labrum can get irritated
- Why it keeps happening: the shoulder is usually being loaded in a way it can’t control well
Once those pieces are clear, rehab becomes far less confusing.
Understanding Your Shoulder Anatomy
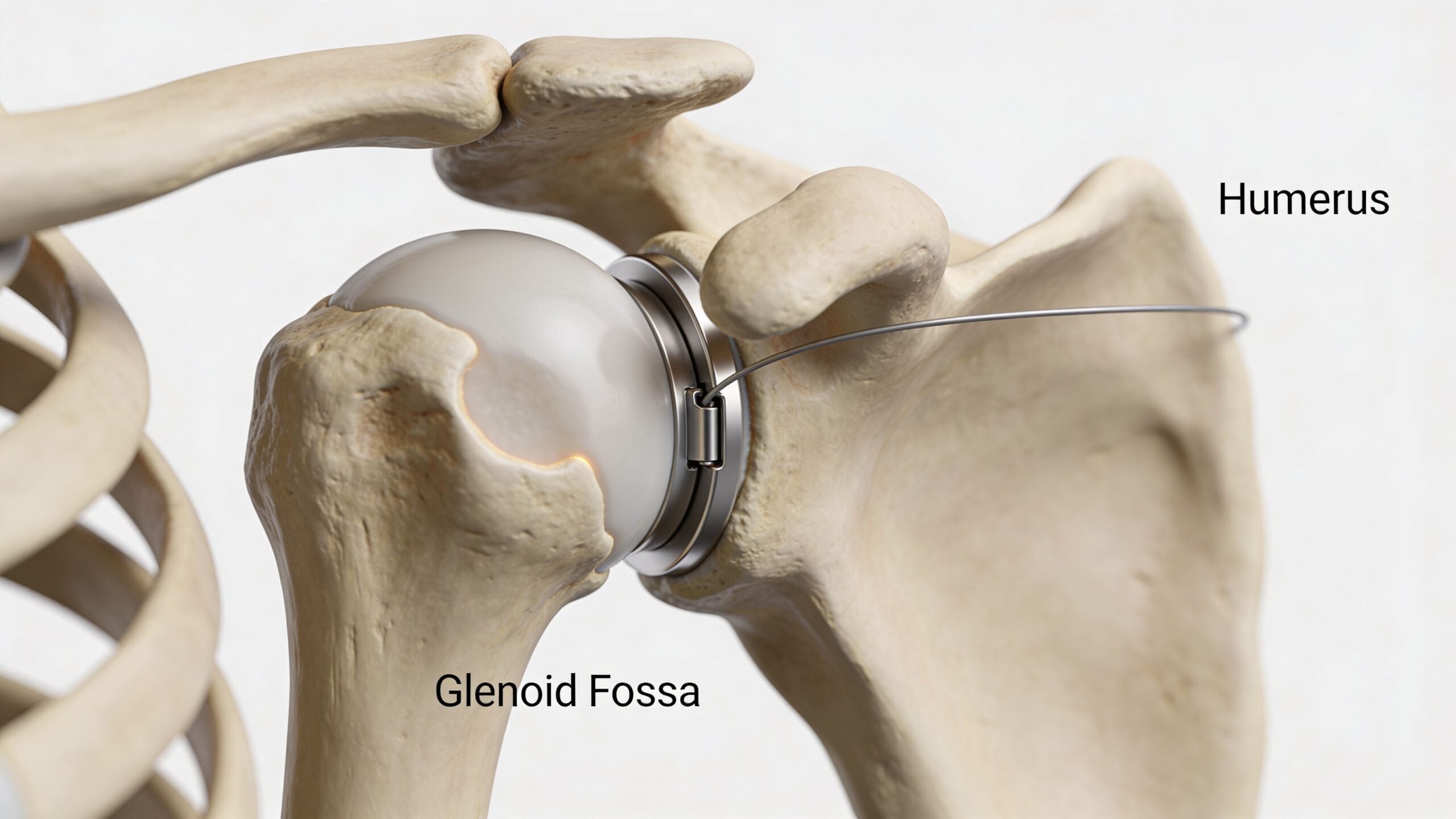
The shoulder works like a ball-and-socket system with a moving platform underneath it. The humeral head is the ball. The glenoid is the shallow socket. The rotator cuff acts like a dynamic centering system that keeps the ball from drifting too far as you move.
In posterior impingement, the tissues that usually get compressed are the infraspinatus and posterior supraspinatus tendons against the posterior superior glenoid rim. This tends to happen during extreme abduction and external rotation, often shortened to ABER in the clinic. That’s the classic “arm up and back” position.
What’s getting pinched
A simple analogy helps. Think of a door hinge at the far end of its swing. If the hinge is loose, the frame is misaligned, and the cable near the edge is tight, the cable gets pinched at the end range. That’s roughly what happens in shoulder posterior impingement.
The main structures involved often include:
- The ball of the shoulder joint: if it glides too far forward, the back side gets crowded
- The posterior rotator cuff: especially the infraspinatus and posterior supraspinatus
- The labrum: the rim of tissue around the socket that can become irritated or frayed
- The shoulder blade: if it doesn’t rotate and tilt well, the mechanics above it worsen
How it differs from the more familiar impingement
The common version people hear about is usually subacromial impingement, where pain is often felt more at the top or side of the shoulder. Posterior impingement is more of a deep back-of-the-joint pain problem.
That distinction changes treatment. A general “shoulder exercise” program may help some people, but it often misses the true drivers of posterior symptoms.
Athletes and non-athletes can both fit this pattern
Posterior impingement is well described in overhead athletes, but it “has also been described in non-athletic individuals,” as noted in this clinical review on internal impingement. That matters because non-athletes are often told their shoulder pain can’t be this diagnosis if they don’t throw, swim, or serve.
That’s not how good diagnosis works. Mechanism matters more than identity. If the movement pattern and symptom location fit, the condition belongs in the discussion.
Common Causes and Primary Risk Factors
Posterior impingement usually develops through one of two routes. The first is repetitive overhead loading in sport. The second is slower, less obvious buildup in people whose daily life repeatedly puts the shoulder into poor mechanics.
The classic athletic pathway
Throwers, swimmers, volleyball players, and tennis players place the shoulder in high-demand overhead positions again and again. During the late cocking and early acceleration phases of throwing, the arm moves into extreme abduction and external rotation. That can compress the posterior cuff against the back of the socket.
Several movement problems commonly travel with this pattern:
- Anterior shoulder laxity: the humeral head can translate too far forward
- GIRD: a loss of internal rotation compared with the other side
- Scapular dyskinesis: the shoulder blade doesn’t upwardly rotate or posteriorly tilt well
- Rotator cuff weakness or poor timing: the ball doesn’t stay centered as efficiently
When those stack together, the shoulder keeps revisiting the same painful pinch.
The overlooked non-athletic pathway
Not everyone with shoulder posterior impingement is throwing a baseball. Some people develop it from repeated reaching, stocking shelves, painting, transferring patients at work, lifting children, or years of sitting with the shoulder blade resting in a poor position.
The shoulder doesn’t care whether the movement came from sport or a job. It responds to repeated stress, poor control, and limited mobility the same way.
Common non-athletic contributors include:
- Rounded posture: the shoulder blade starts in a less favorable position
- Repetitive overhead work: the joint is loaded overhead without enough support
- Stiff posterior tissues: reaching behind the body feels blocked or pinchy
- Age-related movement changes: people lose rotation, thoracic mobility, and cuff endurance over time
If your pain lives deep in the back of the shoulder and flares with arm-up-and-back motions, the diagnosis should be based on that pattern, not on whether you play a sport.
Triggers patients often notice
People usually describe shoulder posterior impingement with very specific aggravating movements. The list is often more useful than a label.
- Reaching back: grabbing the seatbelt, reaching into a back pocket, or pulling something from the back seat
- Overhead loading: pressing, serving, swimming, or placing items on a high shelf
- Late-range rotation: cocking the arm back before a throw or forceful reach
- After-activity soreness: the shoulder feels dull, weak, or “not right” after use rather than only during it
What usually doesn’t work is trying to stretch aggressively into the painful position without fixing the mechanics that created the problem.
Symptoms What Posterior Impingement Feels Like
The hallmark symptom is a deep, aching pain at the back of the shoulder. Not the top. Not the outer arm. Not a surface-level muscle knot. People often place one finger just behind the ball of the shoulder and say, “It hurts right in there.”
Some describe a sharper pinch during the movement and then a dull ache afterward. Others feel a brief loss of power, especially after repeated overhead use. In athletes, that can feel like a “dead arm.” In non-athletes, it may feel more like the shoulder loses confidence and gets irritated by ordinary reaching.
How a clinician separates it from other shoulder pain
A strain is often more tender in the muscle belly and usually ties back to a clear overload event. Bursitis more often creates pain on the side of the shoulder. Neck-related pain can travel down the arm or come with tingling. Posterior impingement tends to stay deep, local, and movement-specific.
A physical therapist puts the pieces together by combining:
- Your history: where it hurts, what position triggers it, and whether overhead use matters
- Movement testing: how the shoulder blade moves, how the ball sits in the socket, and whether internal rotation is limited
- Provocation tests: positions that reproduce the familiar pain pattern
- Imaging when needed: usually to clarify cuff or labral involvement if the exam suggests it
The diagnosis usually comes from a pattern, not from a single painful motion in isolation.
That matters because treatment should match the pattern too.
How Physical Therapists Diagnose This Condition
A good diagnosis starts with listening. Before any test, a physical therapist wants your story. Did the pain begin after repeated overhead work? Does it show up only when the arm is back and rotated? Do you feel weakness, stiffness, or a catching sensation? Those details narrow the field quickly.

The hands-on exam
The next step is a movement exam. A PT checks shoulder range of motion, especially internal rotation. They look at how your scapula moves during lifting and lowering. They test rotator cuff strength and compare side to side. They also check whether the thoracic spine, rib cage, or even hip and trunk control are feeding into the shoulder problem.
One test often used is the posterior impingement sign test. In this test, the arm is passively moved into 90 to 110 degrees of abduction and maximal external rotation, which can reproduce deep posterior shoulder pain. This test has shown 75.5% sensitivity and 85% specificity for detecting the rotator cuff and labral issues associated with the condition, as described in this overview of posterior impingement sign testing.
A positive test doesn’t stand alone. It’s one piece of the puzzle. A negative result can be useful too, especially when the rest of the exam points elsewhere.
What else a PT looks for
Posterior impingement rarely lives by itself. A strong exam also looks for linked impairments.
- Loss of internal rotation: this suggests posterior shoulder tightness or GIRD
- Scapular control problems: poor upward rotation or poor posterior tilt can crowd the joint
- Cuff weakness or endurance deficits: the shoulder may not center well under load
- Joint mobility restrictions: posterior capsule stiffness often changes shoulder mechanics
Hands-on treatment can help clarify what’s driving symptoms. If posterior capsule mobilization immediately improves motion or reduces pain, that tells the clinician something meaningful about the problem. If you want a clearer sense of what that type of care involves, this guide to manual therapy in physical therapy gives a useful patient-friendly overview.
When imaging enters the picture
Imaging can help confirm a suspected cuff or labral issue, especially when symptoms are severe, progress stalls, or the history suggests more structural involvement. But imaging should support the exam, not replace it. Plenty of shoulders show abnormalities on scans that don’t fully explain the pain. The movement exam still drives the plan.
A Phased Approach to Physical Therapy and Rehabilitation
Rehab works best when it follows the shoulder’s real needs, not a random list of exercises. Posterior impingement improves when you reduce the painful compression first, restore motion second, then rebuild control and loading tolerance.

Rehabilitation phases at a glance
| Phase | Primary Goal | Example Interventions |
|---|---|---|
| Phase 1 | Calm pain and reduce mechanical irritation | Activity modification, gentle range of motion, posterior capsule work, early cuff isometrics |
| Phase 2 | Restore clean shoulder mechanics | Internal rotation mobility, scapular control drills, rotator cuff strengthening, thoracic mobility |
| Phase 3 | Return to higher-level function | Overhead progressions, work-specific lifting, throwing or swimming progression, kinetic chain training |
Phase 1 Calm the joint down
At the beginning, the goal isn’t to “push through.” It’s to stop feeding the painful position over and over. That usually means modifying the exact movements that reproduce deep posterior pain.
Early treatment often includes:
- Activity adjustment: reduce repeated arm-up-and-back loading for now
- Gentle mobility: improve motion without forcing into the impingement position
- Posterior capsule work: hands-on mobilization and targeted stretching when indicated
- Pain-limited cuff activation: low-load external rotation and scapular setting drills
Often, patients make their first mistake here. They either shut the shoulder down completely or keep training the same way and hope it settles. Neither strategy works well. The shoulder usually needs smart load reduction, not total rest or full-speed denial.
Phase 2 Fix the mechanics
Once pain is less irritable, rehab needs to become more specific. At this stage, many recoveries either accelerate or stall.
The focus shifts to:
- restoring internal rotation if it’s limited
- improving scapular upward rotation and posterior tilt
- strengthening the rotator cuff so the humeral head stays centered
- improving trunk and rib cage mechanics so the shoulder isn’t doing all the work
Useful exercises often include side-lying external rotation, prone horizontal abduction, rowing variations, wall-based scapular drills, and posterior shoulder stretching when it matches the exam. For readers looking for a broader exercise library, Highbar’s guide to the best exercises for rotator cuff strengthening is a solid companion resource.
Practical rule: If an exercise repeatedly recreates the deep back-of-shoulder pinch, it’s probably too aggressive, too early, or set up poorly.
This phase also includes motor control work. In rehab documentation, that’s often described as neuromuscular reeducation. If you’re trying to understand how that category is defined in clinical billing and plan-of-care language, this explanation of the neuromuscular reeducation CPT code 97112 gives helpful context.
Phase 3 Return to sport, work, and life
The final phase is where rehab has to get honest. Being pain-free on a treatment table isn’t enough if your job requires overhead lifting or your sport demands repeated high-speed rotation.
Return-to-function progressions should match your real demands:
- Workers: repeated reaching, carrying, lifting, and sustained arm positioning
- Lifters: pressing patterns, pulling stability, and eccentric control
- Throwers and swimmers: progressive overhead volume with attention to fatigue
- General active adults: reaching behind, loading overhead, and daily confidence
What doesn’t work at this stage is skipping from band exercises straight back to full intensity. The shoulder has to relearn timing and tolerance under realistic load.
When to escalate care
A focused conservative program generally leads to improvement. But a few situations deserve a higher level of evaluation:
- Traumatic onset: pain began after a fall, dislocation, or forceful injury
- Major weakness: you can’t lift the arm or hold it against gravity well
- Mechanical symptoms: catching, repeated locking, or strong instability sensations
- Plateau despite consistent rehab: progress isn’t happening even with a well-built plan
That doesn’t automatically mean surgery. It means the diagnosis may need another look.
Prevention Strategies and When to See a Specialist
The best prevention plan is not glamorous. It’s consistent. Posterior impingement usually builds from small mechanical problems repeated many times, so prevention depends on keeping those small problems from piling up.
What helps most long term
A shoulder that stays healthy usually has enough mobility, enough cuff strength, and a shoulder blade that moves on time. Most prevention programs revolve around those basics.
- Keep internal rotation available: if the back of the shoulder gets progressively stiffer, mechanics usually worsen
- Train the cuff and scapular muscles regularly: not just when pain starts
- Warm up before overhead loading: your first hard throw, swim set, or overhead work rep shouldn’t be your first shoulder movement of the day
- Manage workload: spikes in volume are a common way symptoms return
If your shoulder is already irritated, be selective with exercise choices. Some movements are useful in one phase and a bad idea in another. This guide on movements to avoid with rotator cuff injury is helpful for understanding how certain positions can aggravate a healing shoulder.
When specialist input makes sense
See a specialist promptly if pain followed a traumatic event, if you have dramatic weakness, or if the shoulder feels unstable in a way that’s getting worse. A specialist evaluation is also reasonable if you’ve done dedicated PT and the pattern still isn’t changing.
For many, there’s no need to panic. They do need a clear diagnosis, a structured rehab plan, and enough patience to let mechanics improve before testing the shoulder at full speed again.
Frequently Asked Questions
Is shoulder posterior impingement the same as regular shoulder impingement
No. The more familiar version usually refers to pain at the top or outer part of the shoulder. Shoulder posterior impingement typically causes pain deep in the back of the joint and is often provoked by the arm being up and rotated back.
Can non-athletes get posterior impingement
Yes. It’s strongly associated with overhead athletes, but clinicians have also described it in non-athletic individuals. Repetitive work tasks, poor shoulder blade mechanics, stiffness, and lifestyle factors can all contribute.
How long does recovery take
Recovery depends on how irritable the shoulder is, how long the problem has been present, and whether the plan addresses the true driver. Some people respond quickly once painful motions are modified and mobility improves. Others need a longer strengthening and movement retraining process before overhead activity feels normal again.
Will I need surgery
Not necessarily. Many people improve with conservative care that restores mobility, cuff strength, scapular control, and functional loading tolerance. Surgery is more likely to enter the discussion if there’s significant structural damage, instability, trauma, or failed progress despite appropriate rehab.
Should I stop all exercise
Usually no. Total rest often makes the shoulder weaker and stiffer. The better approach is to temporarily reduce or modify the movements that recreate the deep posterior pinch while keeping the rest of the body active.
What kind of therapist should I see
Look for a physical therapist who regularly evaluates shoulder pain, overhead mechanics, and return-to-sport or return-to-work progressions. The best rehab plan is specific. It should match your symptoms, your movement exam, and the activities you need to get back to.
If that deep shoulder pain has been lingering, don’t guess your way through it. Highbar Physical Therapy helps patients get a clear diagnosis, a practical rehab plan, and a path back to confident movement with individualized physical therapy care.