A lot of people notice the same odd pattern before they ever hear the word dermatomes. Their thumb goes numb, but the problem is in the neck. Their outer calf burns, but the source is in the low back. Their skin feels “off” in one narrow strip, and they can't tell whether it's a muscle strain, a circulation issue, or something else entirely.
That confusion makes sense. Pain, tingling, and numbness don't always show up where the problem starts. If you've had symptoms that travel, wrap, shoot, or follow a line, a nerve pattern may be involved. That's why physical therapists pay close attention to where symptoms live on the body, especially when someone describes radiating pain.
That Strange Pain That Isn't Where It Seems
A common example is someone who says, “My hand is the problem.” Then the exam shows the hand is only where the signal ends up. The underlying issue may be irritation at a spinal nerve root much closer to the neck.
Think of your nervous system like a wiring map in a house. If a light flickers in the kitchen, the bulb might be fine. The issue could be farther upstream at the switch, breaker, or wiring connection. Your body works in a similar way. A nerve root near the spine sends sensation out to a predictable area of skin. If that nerve root gets irritated, compressed, or inflamed, symptoms can show up anywhere along its territory.
That territory is what clinicians call a dermatome.
Dermatomes help explain why pain can feel misleading. The body part that hurts isn't always the body part that's injured.
For patients, this matters because it changes what “treatment the right spot” means. Rubbing the painful area may help briefly, but it won't solve much if the driver is a nerve root in the spine.
For a PT student, dermatomes are one of the first real bridges between anatomy and clinical reasoning. They turn a vague complaint like “tingling in my fingers” into a focused question: Which nerve root could create that pattern?
Once you see dermatomes as a map, a lot of confusing symptoms start making more sense.
What Exactly Are Dermatomes?
A dermatome is a specific area of skin supplied by sensation from a single spinal nerve root. One clean way to picture it is as a zip code for your nervous system. If a certain patch of skin feels numb, overly sensitive, or painful, that patch can point back to a particular nerve root.
There are 30 dermatomes in the human body, corresponding to 31 pairs of spinal nerves, with C1 typically having no dermatome according to TeachMeAnatomy's overview of dermatomes. That same organization is used in major neurological assessments, including the ASIA scale for spinal cord injury.
Why the map exists at all
This arrangement isn't random. During early development, body tissues form in a segmented pattern. Those segments help organize skin, muscle, and skeletal structures in a way that stays clinically useful later in life. You don't need to memorize embryology to use dermatomes well, but it helps to know that the body was built with this segmental logic from the start.
That's why dermatome patterns are so consistent in practice. They aren't just lines drawn on a textbook figure. They reflect how the nervous system was organized as the body formed.
The main regions
Dermatomes are grouped by spinal level:
- Cervical dermatomes cover much of the head, neck, shoulders, arms, and hands.
- Thoracic dermatomes wrap around the chest and trunk like stacked bands.
- Lumbar dermatomes cover parts of the low back, front of the legs, and parts of the feet.
- Sacral dermatomes cover areas of the pelvis, buttocks, back of the legs, and portions of the feet.
A few examples make the idea easier to hold onto:
- C2 includes the neck, temple, forehead, and occiput.
- C5 includes the deltoid region and front of the arm toward the base of the thumb.
- T2 includes the medial upper arm and nearby chest and upper back regions.
- L1 includes the back, trochanter, and groin.
Why PTs care
Dermatomes matter because they help localize a problem.
If symptoms match a dermatome, a therapist starts thinking about the nerve root. If symptoms don't match a dermatome, the therapist may think more about a peripheral nerve, a local tissue issue, or a non-neurological cause.
Clinical shortcut: Dermatomes don't give the full diagnosis by themselves, but they narrow the search fast.
That's what makes them useful. They turn scattered symptoms into a pattern. And pattern recognition is a huge part of good diagnosis.
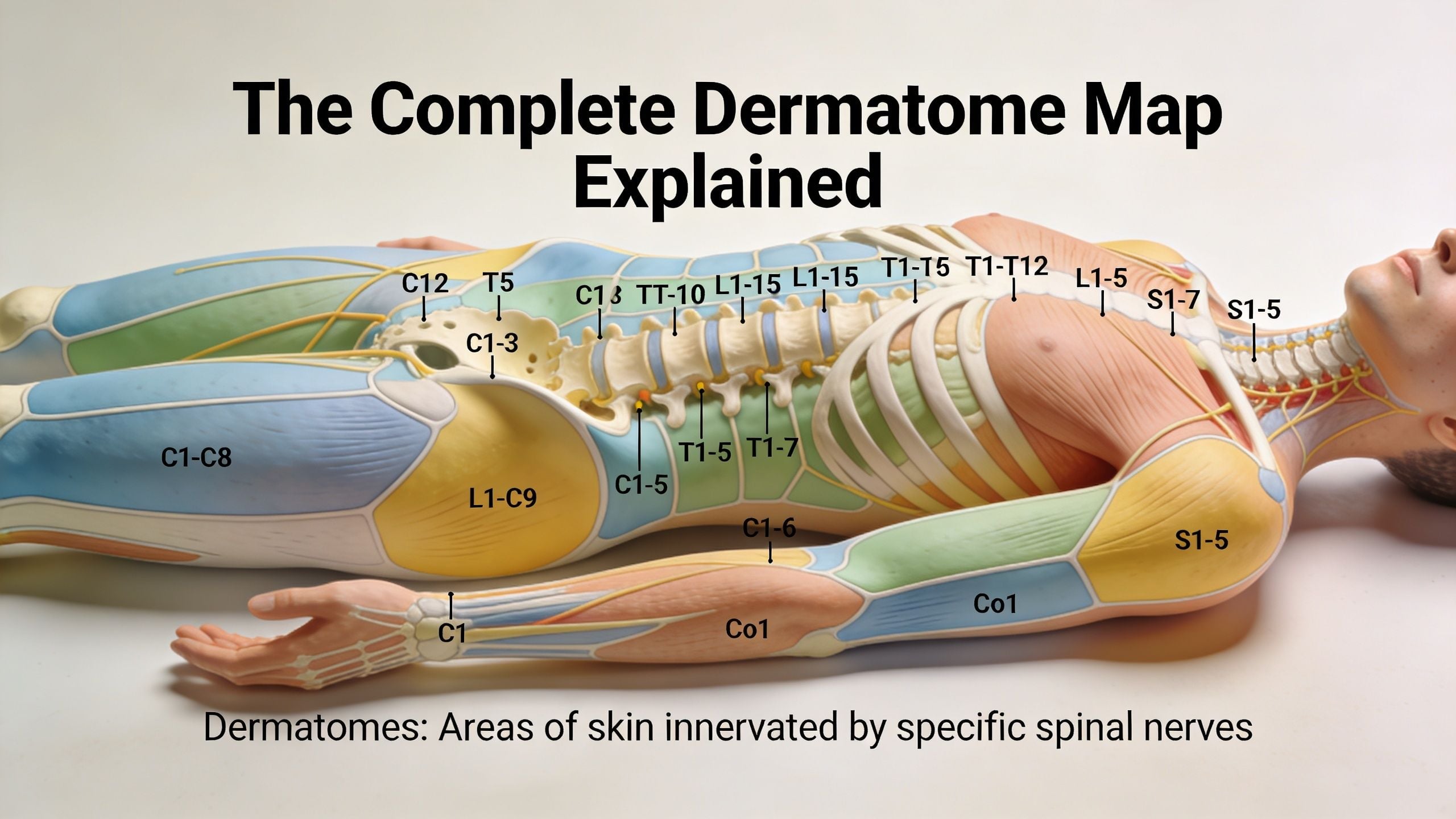
The Complete Dermatome Map Explained
A practical way to organize the dermatome map is to follow the body from head to toe and attach each spinal level to a landmark you can find. That turns a crowded diagram into something a patient can describe and a clinician can test.
Dermatomes work like a wiring map for the skin. If you know which patch of skin connects back to which spinal nerve root, you can make better sense of symptoms that seem to show up far from the true source.
Cervical dermatomes
The cervical dermatomes cover the neck, shoulders, arms, and hands. In the clinic, these levels matter any time neck symptoms travel into the arm or hand.
A few anchors make this region easier to remember:
| Dermatome | Useful landmark |
|---|---|
| C2 | Neck and back of head |
| C5 | Shoulder and lateral upper arm |
| C6 | Upper forearm, thumb, and index finger |
| C8 | Ring and little finger side of the hand |
These landmarks help narrow the starting point of the exam. A person who reports numbness into the thumb and index finger raises suspicion for C6. A complaint focused on the ring and little finger side shifts attention lower, often toward C8.
That does not give the diagnosis by itself. It gives the therapist a better question to test.
Thoracic dermatomes
The thoracic dermatomes wrap around the trunk in horizontal bands, almost like strips around a barrel. This region is often easier to picture on a chart than on a real person, which is why landmarks help.
One useful reference point is T10, which lines up with the area of the belly button. Once that level is fixed in your mind, the thoracic map becomes easier to sort above and below.
Thoracic nerve symptoms may show up as:
- A band of pain around the ribs
- Burning or tingling on one side of the trunk
- A stripe of altered sensation across the chest or abdomen
That pattern matters because trunk pain is easy to misread. People may assume it is a strained muscle, irritated rib, or skin problem when the symptom path points back to a spinal nerve level instead.
Lumbar and sacral dermatomes
The lumbar and sacral dermatomes cover the low back, pelvis, legs, and feet. These are the levels therapists study closely when someone has back pain that spreads into the leg, or leg numbness that seems to come out of nowhere.
A simple way to organize them is by direction of travel on the leg:
- Upper lumbar levels often involve the groin, hip, and front of the thigh.
- Mid and lower lumbar levels often involve the knee, shin, top of the foot, or big toe.
- Sacral levels often involve the back of the leg, outer foot, heel, or saddle region.
The map proves practical. If symptoms run down the leg in a repeatable strip, a therapist starts considering the spine and nerve root, not just the muscles where the pain is felt. That is the same pattern many people notice when dealing with lower back pinched nerve symptoms that travel into the leg.
Real bodies are less tidy than diagrams. Neighboring dermatomes overlap, and one person's map may not match the textbook exactly. That is why PTs use the dermatome map as one piece of the exam, along with strength testing, reflexes, symptom behavior, and movement testing.
Still, the map gives the exam direction. A thumb pattern points one way. A band around the trunk points another. Numbness at the outer foot suggests a different level again. For patients, that helps explain why a therapist asks such specific questions about location. For clinicians, it helps turn a vague symptom like "my leg feels off" into a focused diagnostic path.
How Dermatomes Help Diagnose Common Conditions
Dermatomes become most useful when they stop being a chart and start explaining real symptoms. Two conditions show this clearly: radiculopathy and shingles.

Radiculopathy and the pinched nerve pattern
Take a patient with low back pain who also reports symptoms running down the leg. The first question isn't just “Where does it hurt?” It's “What path does it follow?”
If the pattern fits a dermatome, the working hypothesis shifts toward radiculopathy, meaning irritation or compression of a spinal nerve root. A disc herniation is one common reason that can happen. A narrowed opening around the nerve is another.
A patient might walk in saying:
- the back hurts only a little
- the leg symptoms are worse than the back
- sitting increases the problem
- the pain, tingling, or numbness travels below the knee
That history makes a therapist think beyond a local hamstring or calf issue. If the symptom path is consistent with a dermatome, the spine moves up the suspect list. That's one reason articles on a lower back pinched nerve resonate with so many people. The pain often feels like a leg problem even when the source is in the low back.
Shingles and the one-strip clue
Herpes zoster, or shingles, is one of the clearest examples of a dermatomal pattern. It classically follows a single dermatome, and thoracic and lumbar dermatomes are the most commonly affected, with the rash and pain typically confined to that one nerve territory according to the NCBI Bookshelf review on herpes zoster.
That's why shingles often looks so distinctive. The rash doesn't usually scatter randomly. It tends to stay in one band or region on one side.
A patient may first notice:
- Pain or burning before any rash appears
- Itching or tingling in a narrow area
- A vesicular rash that stays within one dermatome
A symptom that respects a dermatome gives the examiner a strong clue that the nervous system is part of the story.
Why pattern matters more than location alone
Two patients can both point to the leg. One has a calf strain. The other has a compressed lumbar nerve root. The location overlaps, but the pattern differs.
That's the key lesson. PTs don't only ask where symptoms are. They ask how symptoms behave, whether they follow a line, whether they cross sides, and whether they match a known nerve territory.
Dermatomes don't replace the full exam. They sharpen it.
How Physical Therapists Assess Your Sensation
You tell your PT, “My thumb feels numb, but only part of it,” or “The outside of my shin feels strange.” That is the moment the exam gets very specific. A sensation test helps the therapist figure out whether your symptoms match a nerve root pattern, a peripheral nerve, or something less organized.

A dermatome screen works like checking a wiring map. Your skin is the place where the signal shows up, but the problem may start higher up, often near the spine. For patients, that explains why a PT may touch several areas that do not seem related at first. For students, it is a reminder to test the pattern, not just the place the patient points to.
What the test usually looks like
The exam is simple on your end. You close your eyes, relax, and report what you feel.
A PT may use:
- Light touch, often with cotton, tissue, or a fingertip
- Pinprick, to compare sharp sensation in one area versus another
- Side-to-side comparison, checking the same spot on the left and right
- A top-to-bottom scan, looking for where normal sensation changes into altered sensation
The therapist is not grading toughness or pain tolerance. They are listening for consistency. If one patch feels dull, extra sharp, delayed, or oddly “buzzing,” that clue matters because it helps narrow the source.
Terms you may hear during the exam
Some exam words sound technical, but the meanings are straightforward:
| Term | Plain meaning |
|---|---|
| Hypoesthesia | Reduced sensation |
| Hyperesthesia | Increased sensitivity |
| Paresthesia | Tingling, pins and needles, or another unusual sensation |
Simple answers help the most. “Same.” “Less.” “Sharper.” “Tingly.” Those responses give the therapist cleaner information than trying to guess the diagnosis.
Why PTs also test strength and reflexes
Sensation rarely gets assessed by itself. A nerve root problem can change what you feel, how strongly a muscle works, and how a reflex responds. That is why PTs combine dermatomes with myotomes and reflex testing during a neurological screen.
When all three line up, the picture gets sharper. A person with altered thumb sensation, weakness in a matching muscle group, and a changed reflex gives the therapist a much stronger working diagnosis than sensation testing alone. As noted earlier, exam guides commonly describe this combined approach as more useful than any single test by itself.
This part often surprises patients. Their calf tingles, yet the PT checks ankle strength, taps a tendon, and asks whether one side feels different from the other. There is a reason for that sequence. It helps sort out whether the issue acts like a nerve root, a local tissue problem, or a peripheral nerve irritation farther down the arm or leg.
How the findings guide treatment decisions
The exam is not just about naming the irritated level. It helps shape the plan of care.
If your symptoms follow a clear nerve pattern, your PT may focus on positions or movements that reduce pressure on the irritated tissue, add exercises to improve support around the neck or back, and use manual therapy techniques in physical therapy when joint stiffness or guarding is part of the problem. If the pattern does not fit a dermatome, the therapist may look more closely at joints, muscles, circulation, or a peripheral nerve.
For patients doing home exercise work, structured programs such as GrabGains workout plans for back can make more sense once you know why the spine is being treated for pain or numbness felt somewhere else.
For a PT student, the takeaway is simple. Use the dermatome screen to ask better clinical questions. For a patient, the takeaway is just as practical. Your answers during this exam help the therapist decide where the problem is likely coming from, and that changes what treatment is most likely to help.
Physical Therapy for Dermatomal Nerve Pain
When symptoms follow a dermatome, good treatment usually goes after the source of nerve irritation, not just the place where symptoms are felt. If a nerve root in the neck or low back is the driver, spending all your time on the hand or calf misses the bigger issue.
That's why physical therapy often centers on movement at the spine, nerve mobility, and the muscles that support the irritated area. Hands-on care may help reduce stiffness or improve joint motion, and manual therapy in physical therapy often forms part of the plan. But manual treatment is usually only one piece.
What treatment often includes
A PT may build care around a few priorities:
- Directional movement testing to see whether certain positions centralize or reduce symptoms
- Nerve gliding exercises to help the nerve move with less irritation
- Strength work for the trunk, hips, shoulder girdle, or deep neck muscles
- Mobility work for stiff joints and surrounding soft tissue
- Education about posture, loading, sleep positions, lifting, and symptom monitoring
Some patients are surprised by this. Their foot tingles, but the exercise starts at the back. Their fingers burn, but treatment begins with the neck and shoulder mechanics. That approach makes sense once you understand dermatomes.
Why symptom-chasing falls short
Massaging the exact area of tingling may feel good briefly. It rarely changes the nerve root environment by itself.
A better question is, “What mechanical or inflammatory factor is keeping this nerve irritated?” Once you answer that, treatment gets more targeted.
For people rebuilding capacity after a flare-up, general back strengthening can also support recovery. A practical starting point can be structured GrabGains workout plans for back, especially when a clinician has already helped identify which movements are appropriate and which ones should wait.
Rehab principle: Treat the map, but solve the source.
The long-term goal isn't just to calm symptoms. It's to restore movement, build tolerance, and reduce the chance that the same nerve pattern keeps returning.
When to See a Specialist for Your Symptoms
Most dermatomal symptoms aren't an emergency, but some patterns need fast medical attention. The key is watching for signs that suggest more than a routine nerve irritation.
Seek urgent medical care if you have:
- Progressive weakness, especially if it's becoming harder to lift the foot, grip, or raise the arm
- Bowel or bladder changes, especially with numbness in the saddle region
- Symptoms after major trauma, such as a fall, collision, or heavy impact
- Rapidly worsening numbness or severe neurological change
- Eye symptoms with a facial shingles pattern, since trigeminal involvement can threaten vision
If your symptoms are painful, strange, or persistent but not urgent, a physical therapy evaluation is often a smart first step. A good exam can help sort out whether the pattern looks spinal, peripheral, musculoskeletal, or something that needs referral.
The most useful thing you can bring is a clear description: Where does it start? Where does it travel? Is it numbness, burning, pins and needles, or pain? Does it stay in one strip, wrap around the body, or go below the knee or elbow?
That description often tells more than people realize.
If you're dealing with pain, numbness, or tingling that seems to follow a pattern, the next step is a skilled evaluation. The team at Highbar Physical Therapy can assess your symptoms, identify whether a dermatome pattern is involved, and build a plan focused on the underlying source of the problem.
