A runner opens up their stride, feels a sharp grab in the back of the thigh, and suddenly has to shut it down. That moment gets called a “hamstring pull” all the time, but one muscle often deserves the spotlight: the biceps femoris.
For patients, that name can sound overly technical for a very familiar problem. For PT students and new clinicians, it can feel like one more anatomy term to memorize. But this muscle matters because it sits at the crossroads of speed, deceleration, knee control, and lateral thigh pain. When it gets overloaded, the result can be anything from a mild strain to stubborn pain near the outside of the knee.
The biceps femoris also deserves more than generic “hamstring” advice. It has two distinct heads, and they don't behave exactly the same. That difference affects how symptoms show up, how clinicians think through diagnosis, and how exercise selection should change during rehab.
If you're trying to understand a recent injury, or you're treating one, it helps to see the muscle as more than a single rope in the back of the thigh. It's a two-part structure with different attachments, different nerve supply, and different jobs depending on whether the hip, knee, or both are moving.
Introduction to the Biceps Femoris Muscle
The biceps femoris is the outermost hamstring muscle on the back of the thigh. If you place your hand on the back and outside of your thigh, especially when you bend your knee against resistance, you're close to where this muscle becomes easy to feel.
It's important in daily life, not just in sport. You use it when you walk uphill, rise from a chair, climb stairs, slow your leg during walking, and push off while running. It also helps rotate the lower leg outward when the knee is bent, which becomes relevant in cutting, turning, and stabilizing the knee.
What makes it clinically interesting is that it isn't one uniform structure. It has a long head and a short head. The long head crosses both the hip and the knee, while the short head only crosses the knee. That means one part can be stressed by hip position and the other can't.
The quickest way to get lost with hamstring injuries is to treat all posterior thigh pain as the same problem.
That's why a person may say, “I pulled my hamstring,” yet the underlying issue could be a sprint-related strain in the long head, irritation near the fibular head, referred pain from the back, or symptoms tracking with sciatic nerve irritation.
For a patient, understanding the biceps femoris answers a simple question: “Why does this spot keep flaring up?” For a clinician, it answers a more useful one: “Which structure is overloaded, and what movement is provoking it?”
Anatomy and Biomechanics of the Biceps Femoris
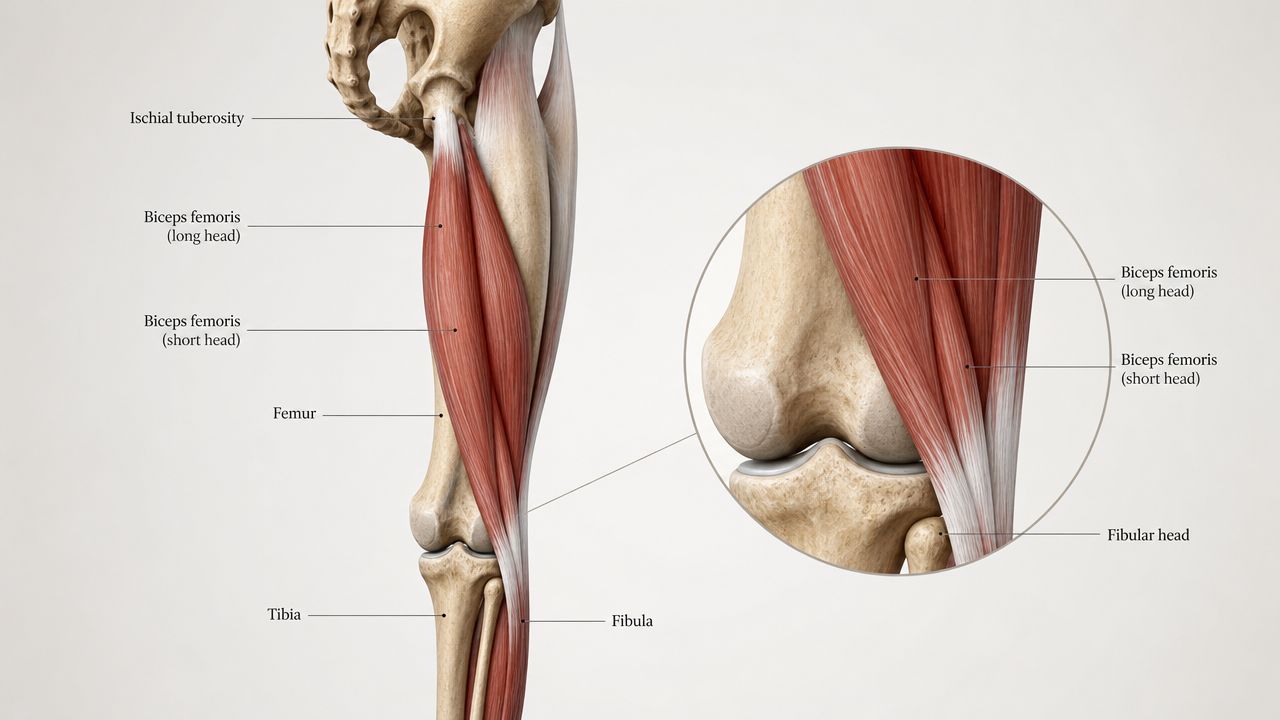
The biceps femoris sits on the lateral, or outer, side of the hamstring group. It runs from the pelvis and femur down toward the outside of the knee, where both heads insert on the head of the fibula. According to Physio-pedia's biceps femoris anatomy reference, the long head arises from the ischial tuberosity, while the short head arises from the linea aspera and lateral supracondylar line of the femur.
Two heads, two jobs
The easiest way to think about it is this:
| Part | Starts from | Crosses | Main contribution |
|---|---|---|---|
| Long head | Ischial tuberosity | Hip and knee | Hip extension and knee flexion |
| Short head | Femur | Knee only | Knee flexion |
Because the long head crosses two joints, it changes length with both hip and knee motion. That gives it a bigger role in running, hinging, and controlling the leg when it swings forward. The short head is more limited mechanically, but it still matters for knee function and local symptom patterns.
Both heads also help with external rotation of the lower leg when the knee is flexed. That's one reason pain near the biceps femoris can show up during twisting or direction changes, not just straight-line sprinting.
Why the nerve supply matters
One detail many people miss is the nerve supply. The same Physio-pedia reference notes that the long head is innervated by the tibial division of the sciatic nerve, while the short head is innervated by the common fibular division.
That's more than a trivia point. It helps explain why symptoms don't always behave uniformly across the whole muscle. For a clinician, unusual weakness or exam findings can raise questions about whether the issue is muscular, tendinous, or related to nerve involvement. If you want a nearby anatomy comparison, the piriformis muscle also matters because it sits close to the sciatic nerve and can complicate posterior hip and thigh symptoms.
A better way to picture its function
Think of the biceps femoris long head like a cable that spans two hinges. If the hip flexes while the knee straightens, the cable gets tension from both ends. That's exactly the sort of setup that makes a muscle vulnerable when it has to produce force while lengthening.
The short head is different. It only responds to what the knee is doing. So if a person has pain that spikes mostly with knee-driven tasks, especially around the outer back corner of the knee, the short head and distal tendon deserve closer attention.
Common Biceps Femoris Injuries and Mechanisms
In repeated sprint sports, the biceps femoris is the most frequently injured hamstring muscle. A review in the National Library of Medicine article on hamstring injury mechanisms notes that the eccentric phase of running is a key risk period, and that 79% of hamstring injuries involve the biceps femoris.
That statistic fits what clinicians see all the time. The athlete isn't usually hurt during a slow jog. The problem shows up when the leg is moving fast and the hamstrings have to control it just before the foot contacts the ground.

Strain during high-speed running
The classic mechanism is a strain. In plain language, the muscle is trying to brake the swinging leg while it's being stretched. That's what “eccentric loading” means here. The muscle is active, but it's lengthening instead of shortening.
The long head crosses both hip and knee. During late swing in running, the hip is flexed while the knee is extending. That combination lengthens the long head from both directions at once.
Practical rule: The faster the running speed, the less room there is for weak braking capacity.
Patients often describe a sudden sharp pain, a grabbing sensation, or a feeling that someone kicked them from behind. In milder cases, they can keep moving but feel tightness and loss of speed. In more severe cases, they stop immediately.
Distal tendon pain and lateral knee symptoms
Not every biceps femoris problem is a dramatic sprint strain. Some people develop pain lower down, near the outside of the back of the knee. That pattern can look like “knee pain,” but the distal biceps femoris tendon may be part of the picture.
Anatomy's clinical utility is demonstrated by a cadaveric study described in this PubMed summary of distal biceps femoris insertion anatomy which found that the insertion is more complex than the old “fibular head only” description. It includes additional slips and connections to nearby posterolateral structures. That helps explain why local irritation can overlap with lateral knee pain and posterolateral corner symptoms.
Pull, tear, or something else
People often use “pull” and “tear” interchangeably. In practice, clinicians think more in terms of severity, location, and function loss. If you want a plain-language breakdown of how these terms are commonly used, this guide can help you compare muscle tear and pull symptoms.
Common patterns include:
- Mid-thigh strain from sprinting or rapid acceleration.
- Distal tendon irritation near the outer back portion of the knee.
- Avulsion-type injury when the tendon pulls away from bone, usually after a more forceful event and with more dramatic loss of function.
The mechanism tells you a lot. A sudden high-speed event points toward strain. Gradual irritation near the outside of the knee suggests tendon overload or repeated traction at the distal attachment.
Diagnosis and Clinical Signs
Most biceps femoris injuries can be suspected from the history before any special test begins. The pattern matters. Sudden pain during sprinting, acceleration, or a quick deceleration points in one direction. Pain that builds during running, hills, or repeated knee flexion work may point in another.
What the patient often notices
Patients commonly report:
- Sharp posterior-lateral thigh pain during a fast movement
- Tightness or cramping that doesn't feel like normal fatigue
- Weak push-off or reduced stride confidence
- Bruising or tenderness after the first day or two
- Pain near the outer back knee in more distal cases
A loud pop, visible deformity, or inability to bear weight raises concern for a more significant injury.
What a PT is trying to sort out
A physical therapist usually wants to answer three questions.
First, where is the pain generator? The biceps femoris can hurt in the upper thigh, mid-belly, or distally near the fibular head. Second, how irritable is it? Some people only hurt with sprinting, while others hurt with walking or sitting. Third, is this really the biceps femoris at all?
That last question matters because posterior thigh pain has several lookalikes. Referred pain from the lumbar spine, sciatic irritation, and symptoms from nearby structures can all mimic a hamstring strain. If the pain burns, radiates, or travels below the knee, it helps to understand what radiating pain means and why the source may not be the thigh muscle itself.
Pain in the back of the thigh isn't automatically a hamstring injury. The movement exam usually tells the real story.
Exam findings and imaging
On exam, a clinician may reproduce symptoms with resisted knee flexion, palpation along the outer hamstring, or lengthened hamstring testing. They'll also look at gait, single-leg control, hip strength, and lumbar screening.
Imaging isn't always necessary. Many straightforward strains are managed based on history and physical exam. MRI or ultrasound becomes more useful when the diagnosis is unclear, symptoms are severe, return-to-sport planning is complicated, or an avulsion is suspected.
Grading still has value, but function matters more than labels alone. A person with a “mild” strain who can't tolerate load isn't ready for the same program as someone with minor soreness and near-normal strength.
Evidence-Based Rehabilitation Protocols
Rehab works best when it follows the actual demands placed on the muscle. The goal isn't just to make pain settle down. The goal is to restore the biceps femoris so it can handle braking, hip extension, knee flexion, and speed again.

Phase one settles symptoms without shutting everything down
Early rehab is about protection and optimal loading, not complete rest unless the injury is severe. The irritated tissue needs calm, but it also needs the right amount of movement.
Early priorities often include:
- Compression and relative rest if walking is painful
- Short, easy range movements to avoid stiffening up
- Pain-limited isometrics such as gentle heel digs
- Normal walking mechanics as soon as tolerated
If pain spikes with every step, a temporary reduction in activity is reasonable. If a patient can walk with only mild discomfort, total inactivity usually isn't helpful.
A simple example is a supine heel dig. The knee is bent, the heel presses into the floor, and the hamstring contracts without visible motion. That gives the muscle some load without forcing lengthening under stress.
Phase two restores motion and basic strength
Once the acute irritation settles, the work becomes more active. The aim is to regain confidence in bending the knee, extending the hip, and controlling pelvic position.
Good options here include:
- Bridge variations starting double-leg, then single-leg
- Standing hamstring curls with light resistance
- Hip hinge drills using a dowel or wall tap
- Low-load slider work if tolerated
This phase is also where glute strength and trunk control matter. If the glutes aren't contributing well during hip extension, the hamstrings often end up doing too much. That doesn't mean glute weakness causes every hamstring injury, but it does mean movement strategy matters.
Phase three builds the strength that sport actually needs
At this stage many people under-rehab. Pain is better, walking is fine, and they assume they're ready. But the biceps femoris often gets hurt when it has to absorb force while lengthening. Rehab has to reflect that.
Useful strengthening choices include:
| Exercise | Main rehab value | Common use |
|---|---|---|
| Romanian deadlift | Hip hinge strength in a lengthened position | Builds posterior chain tolerance |
| Single-leg RDL | Hip control plus asymmetry training | Exposes side-to-side deficits |
| Slider leg curl | Hamstring strength with progressive lengthening demand | Bridges basic to advanced loading |
| Nordic hamstring exercise | Heavy eccentric loading | Key for higher-speed athletes |
One important nuance is exercise setup. Research summarized in the Journal of Sports Science and Medicine Nordic hamstring paper found that performing the Nordic hamstring exercise on an inclined platform with a shallow knee flexion angle can make biceps femoris long head activation equivalent to semitendinosus. That's a useful detail when the goal is not just “hamstring strength,” but more targeted loading of the long head.
For the patient, that means two Nordics can feel similar but train the tissue differently. For the clinician, it means setup matters.
If a sprint athlete keeps re-injuring the outer hamstring, “do hamstring exercises” is too vague to be a plan.
Phase four prepares the leg for speed and unpredictability
Strength alone isn't enough. The final stage needs to reconnect the muscle to the movements that caused trouble in the first place.
That often includes:
Progressive running drills
Start with submaximal strides, then build speed exposure gradually.Plyometric tasks
Skips, bounds, and low-level hops teach the leg to store and release force again.Change-of-direction work
Especially important when symptoms showed up during cutting or deceleration.Sport-specific integration
Position drills, ball work, or repeated accelerations depending on the athlete.
This is also where head-specific thinking becomes useful. Mechanistic work reported in this PMC article on biceps femoris load sharing found that after dissection of intermuscular connections, biceps femoris long-head shear modulus increased by 62.2% while the short head decreased by 36.0%, suggesting meaningful load-sharing between heads. Clinically, that supports the idea that a generic hamstring program may not challenge each part of the biceps femoris equally.
In real practice, that means one person may tolerate bridges and curls but still fail when speed and long-head demand increase. Individualization matters. A clinic-based program, a home plan, or care through a provider such as Highbar Physical Therapy can all work if the loading is progressive and specific.
Return to Play and Injury Prevention Strategies
The goal isn't just to get rid of pain. It's to return to running, lifting, or sport without the constant feeling that the muscle could grab again on the next hard effort.

What reduces recurrence risk
The strongest prevention plans are boring in the best way. They rely on consistency.
A useful foundation includes:
Dynamic warm-up before speed work
Leg swings, marching, skipping, and progressive build-up runs prepare the tissue for fast lengthening loads better than passive stretching alone.Regular eccentric hamstring work
Keep at least one lengthened hamstring strength exposure in the weekly plan once symptoms have resolved.Hip and trunk control
Pelvic control influences how much stretch and load the posterior thigh sees during running.Speed exposure
Athletes who never touch faster running in training often struggle when forced to reach it in competition.
Recovery habits matter too. Sleep, total training load, and basic nutrition all influence how well tissue adapts. For patients who want a simple, food-focused overview, this article on Gym Snack for muscle recovery is a practical starting point.
What return to play should actually mean
Return to play shouldn't mean “I can jog without pain.” It should mean the person can perform the movements their sport or activity demands, at the speed and confidence those movements require.
A solid return-to-play decision usually includes:
| Question | Why it matters |
|---|---|
| Can they sprint or accelerate without guarding? | Sprinting is often the original injury mechanism. |
| Can they produce force in a lengthened position? | This is where the muscle often fails under demand. |
| Can they repeat efforts without symptoms building? | One good rep doesn't prove readiness. |
| Do they trust the leg again? | Hesitation changes mechanics and can shift load elsewhere. |
The absence of pain is only one checkpoint. It is not the finish line.
For runners, this often means a graded plan that moves from easy runs to strides, then faster intervals and sharper changes in pace. If you want broader guidance around training habits, how to prevent running injuries offers a useful framework.
When to See a Physical Therapist
Some hamstring issues calm down with short-term activity modification. Others linger because the original diagnosis was incomplete or the rehab never matched the demands of the injury.
You should get evaluated promptly if you felt a loud pop, noticed major bruising, can't walk normally, or see a visible change in the shape of the back of the thigh. Those signs raise concern for a more significant tear or tendon injury.
You should also consider seeing a PT if the pain keeps returning, shifts toward the outside of the knee, or seems mixed with numbness, tingling, or radiating symptoms. Those patterns can point to a more layered problem than a simple strain.
For people starting from scratch, a basic home program can help with general strength. If you want a simple starting point, Zing Coach's beginner guide offers approachable introductory exercises. But if symptoms are sharp, stubborn, or tied to running and sport, generic beginner work usually won't be enough.
A physical therapist can identify whether the problem is the long head, the short head, the distal tendon, or something outside the biceps femoris entirely. That changes the exercise plan, the return-to-sport timeline, and the risk of getting hurt again.
If your hamstring pain isn't improving, or you want a clearer plan for returning to running or sport, Highbar Physical Therapy can help you get evaluated, understand what's driving your symptoms, and build a rehab program that fits your goals.
