You feel pain deep in the buttock, maybe with tingling down the leg, and someone tells you, “It's probably your piriformis.” Another person says it's sciatica. A third says to stretch more. That mix of advice is common, and it's also where people get stuck.
The piriformis is real. Piriformis-related pain is real. But the story is often more complicated than “one tight muscle.” If you understand where the piriformis sits, what it does, and how clinicians sort it from back-related nerve pain, the next steps get much clearer.
The Piriformis Muscle Explained
The piriformis is a small muscle, but it has an outsized job. I often describe it as a rudder deep in the back of the hip. It doesn't generate the biggest force, but it helps guide motion and keep the joint steady when you walk, turn, climb stairs, or change direction.
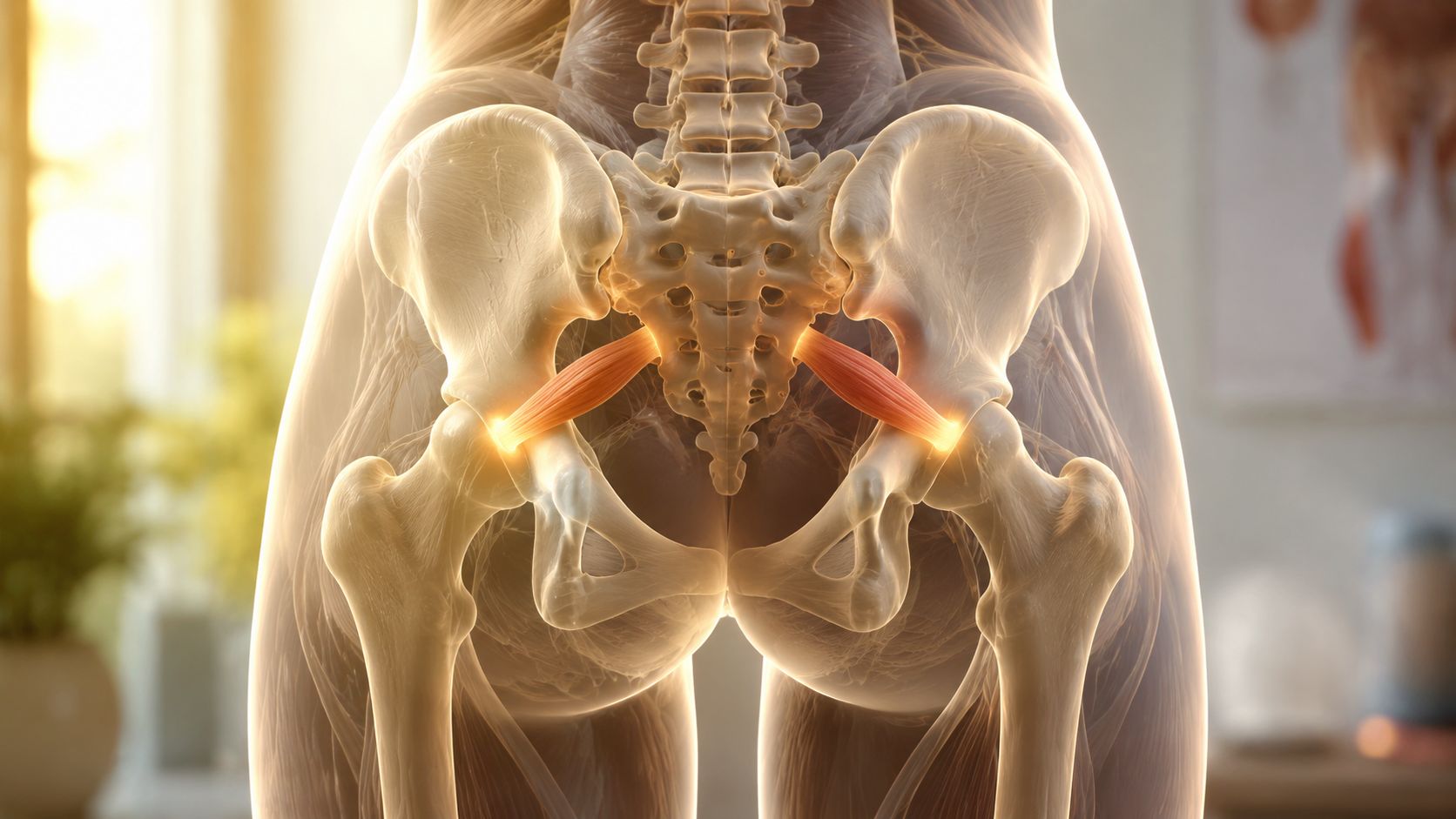
Anatomically, the piriformis is a flat, oblique, pyramidal-shaped deep gluteal muscle that starts on the front surface of the sacrum and attaches to the greater trochanter of the femur, the bony prominence near the top of the thigh bone. It's classified as one of the six short external rotators of the hip and helps stabilize the hip joint, externally rotate the thigh, and abduct the thigh when the hip is flexed, as described in this anatomical review of the piriformis muscle.
Where it is and why that matters
The piriformis runs from the sacrum to the femur, crossing behind the hip joint. That path matters because it places the muscle in the deep gluteal region, very close to the sciatic nerve as the nerve exits the pelvis.
That close relationship is why a small muscle can create big symptoms. When the piriformis becomes irritated, overactive, or involved in a broader deep hip problem, the nearby nerve can become sensitive too.
What the piriformis actually does
A lot of people hear that the piriformis “rotates the hip” and stop there. That's only part of the picture.
Its main roles include:
- Hip stability: It helps keep the head of the femur centered in the hip socket during movement.
- External rotation: When your hip is more extended, it helps turn the thigh outward.
- Abduction in flexion: When your hip is bent, it helps move the thigh away from the body.
That last point confuses people. The piriformis doesn't behave the same way in every position. Its line of pull changes with hip angle, which is one reason symptoms can show up during sitting, squatting, running, or crossing the legs.
Practical rule: A muscle can be small, deep, and still matter a lot if it affects both joint control and a nearby nerve.
Why people notice it only when it hurts
You won't usually feel your piriformis when it's doing its job well. You notice it when movement becomes guarded, sitting gets uncomfortable, or the body starts compensating.
Common examples include:
- Sitting for long periods: The back of the hip gets compressed.
- Running or cutting: The muscle has to help control rotation and stabilize the hip.
- Getting out of a car: The combination of hip flexion and rotation can provoke symptoms.
That's why piriformis issues rarely exist in isolation. The muscle works with the gluteals, the rest of the deep hip rotators, the pelvis, and the low back. If one part isn't doing its share, the piriformis often picks up extra work.
What is Piriformis Syndrome
Piriformis syndrome is the term commonly used when the piriformis contributes to irritation or compression of the sciatic nerve. When that happens, pain may stay in the buttock, or it may travel down the back of the leg in a pattern that feels a lot like sciatica.
Clinically, people often describe a deep ache in the buttock that gets worse with sitting, driving, bicycling, or running, sometimes with tingling or other abnormal nerve sensations. Stepwise management usually starts with conservative care such as physical therapy, as outlined in this evidence-based discussion of piriformis syndrome and management.
What people often get wrong
The most common misunderstanding is that piriformis syndrome always means the muscle is only “tight.” Sometimes tightness is part of the picture, but not always.
Symptoms can be influenced by:
- Prolonged sitting: Compression in the deep hip can build up over the day.
- Repetitive loading: Running, cycling, and similar activities can irritate the area.
- Direct trauma: A fall onto the buttock can sensitize the muscle and nearby tissues.
- Anatomical variation: In some people, the sciatic nerve courses in a way that changes its relationship to the piriformis.
If your symptoms show up after sitting and ease somewhat once you move around, that pattern can fit a deep gluteal problem. If that sounds familiar, this guide on painful hips after sitting may also help you connect the dots.
What symptoms tend to feel like
People usually don't point to the center of the low back first. They point to the buttock.
You might notice:
- A deep buttock ache
- Pain with sitting or getting up from sitting
- Pain during driving or on a bike
- Tingling, burning, or numbness down the back of the thigh
- Symptoms that mimic a pinched nerve from the back
Piriformis-related pain can feel like sciatica, but that doesn't automatically mean the problem started in the spine.
That distinction matters because treatment depends on the source. If the nerve is irritated in the deep gluteal space, the plan looks different than it would for a disc-related lumbar problem.
Why diagnosis matters
A lot of people lose time by chasing the wrong solution. They stretch aggressively because someone told them the piriformis is tight, but the actual driver may be poor hip control, nerve sensitivity, sitting tolerance, or another structure in the deep gluteal region.
That's why a good exam matters more than a label. “Piriformis syndrome” can be a useful shorthand, but it's only helpful if the clinician also asks what is provoking the muscle and the nerve in the first place.
Piriformis Syndrome vs Sciatica From the Back
Most patients understandably find this confusing. Sciatica describes symptoms along the sciatic nerve, but it doesn't identify the exact source. The source might be the lumbar spine, or it might be the deep gluteal space around the piriformis and nearby structures.
Modern clinicians often use the term deep gluteal syndrome for sciatic nerve entrapment in the gluteal space from multiple possible causes, not just the piriformis alone. A review in Practical Neurology notes that the most common pelvic entrapment site in large studies was beneath the piriformis at 67.8%, which is one reason many experts now think beyond the muscle itself when symptoms are persistent or unclear, as discussed in this review on deep gluteal syndrome and piriformis syndrome.
Why the terms get mixed together
If you have pain in the buttock and down the leg, someone may say “sciatica.” They're describing the symptom pattern, not the diagnosis.
If the nerve is being irritated in the deep hip region, that may be called piriformis syndrome or deep gluteal syndrome. If the nerve root is irritated as it exits the spine, that's lumbar radiculopathy, which many people also call true sciatica.
Symptom Comparison Deep Gluteal Pain vs Lumbar Sciatica
| Symptom/Trigger | Deep Gluteal Syndrome (e.g., Piriformis) | Lumbar Radiculopathy (True Sciatica) |
|---|---|---|
| Primary pain area | Often starts deep in the buttock or posterior hip | Often starts in the low back, buttock, or both |
| Sitting tolerance | Sitting often aggravates symptoms quickly | Sitting may aggravate symptoms, but patterns vary |
| Driving or cycling | Common triggers because of sustained hip position and compression | Can aggravate symptoms, but often depends more on spinal loading |
| Bending and lifting | May or may not be provocative | More often aggravated by spinal flexion, lifting, or coughing/sneezing |
| Local buttock tenderness | Often present | Less central to the picture |
| Nerve symptoms below the knee | Can happen, but not always | Often more classic nerve-root distribution |
| Movement clue | Hip rotation, prolonged sitting, and single-leg control may reproduce symptoms | Repeated spine movements may reproduce or change symptoms |
| Clinical interpretation | Suggests entrapment or irritation in the deep gluteal space | Suggests irritation of a lumbar nerve root |
What a clinician listens for
A physical therapist won't rely on one symptom alone. We look for the pattern.
For example:
- Buttock-first pain with sitting intolerance leans the exam toward the deep gluteal region.
- Back pain with leg symptoms changed by spinal movement leans more toward the lumbar spine.
- Mixed findings are common, especially when someone has been compensating for a while.
That's why self-diagnosis can be tricky. The location of pain matters, but so do the movements and positions that make it better or worse.
The key question isn't just “Do I have sciatica?” It's “Where is the nerve being irritated, and why?”
When you answer that well, the treatment plan becomes much more precise.
How Physical Therapists Diagnose Piriformis Pain
A piriformis evaluation usually starts with a conversation that feels simple but tells us a lot. Where is the pain? When did it start? Is it worse with sitting, walking, stairs, running, or getting in and out of the car? Does it stay in the buttock, or does it travel?
Then we watch you move. A physical therapist looks at how you stand, squat, walk, balance, rotate, and load one leg at a time. We also examine the low back and the hip because piriformis pain can overlap with both.
What the exam usually includes
A thorough exam may involve:
- Hip and lumbar range of motion: We check whether the hip, spine, or both reproduce symptoms.
- Strength testing: Weakness in the gluteals or poor pelvic control can shift extra work to the deep hip muscles.
- Palpation: We assess whether pressure in the deep buttock reproduces your familiar pain.
- Provocative positions: Specific movements can help narrow down whether the source is in the gluteal space or higher up at the spine.
- Neural screening: We assess how the sciatic nerve responds to movement and position.
If nerve symptoms seem confusing, it also helps to understand how clinicians map areas of sensation. This overview of dermatomes gives useful context for why pain from the back can sometimes resemble pain from the hip.
Why one-size-fits-all diagnosis doesn't work
The piriformis sits deep under layers of tissue, and there's real anatomical variation from person to person. CT-based anatomy work found that the distance from the skin to the piriformis averaged between 5.2 cm and 6.6 cm, which helps explain why assessment and treatment need to be individualized, as shown in this clinical anatomy study of piriformis measurements.
That variability matters in the clinic. Two people can both say, “I have pain in the buttock when I sit,” and still need different treatment plans.
What patients should expect
Individuals often feel relieved when they realize the diagnosis isn't a guessing game. It's a process of matching your story with movement findings.
A good PT exam doesn't just ask where it hurts. It asks what the body is doing when it hurts.
That's often the turning point. Once the source is clearer, treatment can move beyond generic stretching and toward a plan designed for your movement pattern.
Effective PT Treatment for Piriformis Syndrome
You sit through a commute or get up after a workout, and the familiar ache grabs deep in the buttock again. At that point, the question is usually simple. Should you stretch more, rest more, or worry that it is really sciatica from your back?
Treatment works best when it answers that question first, then matches the plan to the actual driver of symptoms. In some people, the piriformis is part of the problem. In others, the deeper issue is irritation in the deep gluteal space around the sciatic nerve, which is one reason many clinicians now use the broader term deep gluteal syndrome. That is also why a good PT plan goes well beyond "just stretch it."

Settle the area down first
Early treatment focuses on reducing the irritation that keeps the hip and nerve on edge. If the tissue is already sensitive, pushing hard into exercise too soon can keep the cycle going.
A PT may use:
- Manual therapy: Hands-on treatment to the deep gluteal region can reduce guarding and make movement feel less threatening.
- Load modification: Temporary changes to running, cycling, hills, lifting, or prolonged walking can calm symptoms without stopping activity completely.
- Sitting changes: Shorter sitting bouts, a different seat setup, and regular standing breaks often help when compression is part of the problem.
Massage can help during this stage, especially if nearby muscles are tightening up to protect the area. For a practical self-care overview, these Stillwaters Healing & Massage tips on sciatica can be a useful complement between therapy visits.
Restore motion carefully
The piriformis and nearby tissues respond best to the right amount of motion, not the most motion. A sensitive nerve behaves a bit like an irritated phone charger cable. Repeatedly yanking on it does not make it work better.
That is why PTs usually dose mobility work with care. A gentle seated stretch may help one person. Another person does better with hip rotation drills, breathing-based mobility, or nerve glides that improve movement without provoking symptoms.
Common options include:
- Gentle piriformis stretching: Helpful when it eases tension and does not reproduce sharp, zinging, or spreading pain.
- Hip rotation mobility drills: These improve how the ball and socket joint shares motion.
- Nerve glides: Useful when the sciatic nerve is moving poorly but should be done in a controlled way, not forced.
Build support around the deep hip
Pain often settles faster when the larger hip muscles start doing more of the work they are supposed to do. If the pelvis wobbles or the thigh rotates inward too easily during walking, stairs, squatting, or running, the piriformis can end up acting like a small helper trying to do a bigger muscle's job.
That is where strengthening matters.
A PT program often includes:
- Bridges: To improve hip extension strength and reduce overuse of the smaller deep rotators.
- Side-lying hip work or clamshells: Chosen carefully so you strengthen without reinforcing compensation.
- Single-leg balance and control drills: To expose the movement habits that often keep symptoms recurring.
- Lateral hip strengthening: Better control from the gluteal muscles can decrease stress in the deep buttock region.
These gluteus medius exercises for hip stability are a good example of why side-hip strength matters so much in lasting recovery.
Retrain the movements that keep provoking symptoms
Exercises alone are rarely enough if the same aggravating pattern shows up all day. PT treatment usually includes changes to the positions and tasks that keep reloading the area.
That may include reviewing:
- How you sit and how long you stay there
- How you warm up before exercise
- Whether recent training volume increased too quickly
- How you squat, hinge, climb, run, or push off one leg
- Whether your symptoms behave more like deep gluteal irritation or true lumbar sciatica
This part matters because lasting improvement depends on tolerance in real life, not just in the clinic.
Highbar Physical Therapy provides outpatient physical therapy for musculoskeletal pain and movement limitations, including individualized evaluation and exercise-based treatment.
Relief tends to come faster when the treatment matches the source of irritation. Sometimes that source is local tissue sensitivity. Sometimes it is weak hip control. Sometimes the sciatic nerve is the main issue. Often it is a mix.
A well-built plan usually progresses in stages. First, calm the symptoms enough to move with less pain. Next, restore motion and muscle control. Then build enough strength and endurance that sitting, lifting, training, and daily activity stop setting the problem off again.
Prevention and When to See a Physical Therapist
If piriformis pain has shown up once, prevention matters because the same movement and loading habits often bring it back. The goal isn't to avoid activity. The goal is to keep the hip moving well, the glutes doing their share, and the nerve from getting repeatedly irritated.

What helps lower the risk
Most prevention strategies are simple, but they work best when you build them into your routine.
- Break up long sitting periods: Stand, walk, or change position regularly if your symptoms tend to build while seated.
- Warm up before exercise: Start with dynamic movement so the hip and trunk are ready before speed, hills, or heavy lifting.
- Keep hip strength in your program: Don't rely on stretching alone.
- Watch your training spikes: Sudden increases in mileage, intensity, or volume can aggravate the deep hip.
- Adjust your workspace: Seat height, posture, and movement breaks can make a real difference if desk time is a major trigger.
When self-care isn't enough
A short flare that improves with simple changes isn't unusual. But some patterns deserve a professional exam sooner rather than later.
Consider seeing a physical therapist if:
- Pain keeps going and isn't settling
- Symptoms are spreading farther down the leg
- Sitting, sleeping, or walking is getting harder
- You feel weakness, persistent numbness, or loss of control
- You're not sure whether the problem is your hip or your back
Those situations usually don't improve by guessing. They improve when someone identifies the source and gives you a plan matched to it.
If pain is changing how you sit, walk, exercise, or sleep, it's time for a proper movement exam.
Early treatment can prevent a temporary irritation from turning into a longer cycle of guarding, compensation, and recurring nerve symptoms.
Frequently Asked Questions About Piriformis Pain
| Question | Answer |
|---|---|
| Can piriformis pain cause symptoms below the knee? | Yes, it can. If the sciatic nerve is irritated, symptoms may travel farther down the leg. That said, symptoms below the knee also raise the question of whether the low back is involved, which is why a full exam matters. |
| Is stretching the piriformis always a good idea? | No. Stretching can help some people, but it isn't automatically the right answer. If stretching increases tingling, burning, or sharp radiating pain, it may be aggravating a sensitive nerve rather than helping the muscle. |
| What's the difference between piriformis syndrome and deep gluteal syndrome? | Piriformis syndrome refers specifically to the piriformis contributing to sciatic irritation. Deep gluteal syndrome is a broader term that includes other causes of sciatic nerve entrapment in the gluteal space. |
| Can piriformis pain feel like a disc problem? | Absolutely. Buttock pain, leg pain, and tingling can overlap with lumbar radiculopathy. The difference usually comes from the full symptom pattern and movement exam, not from one symptom alone. |
| Will rest fix it? | Short-term unloading can calm symptoms, but rest alone usually doesn't solve the reason it started. Most people do better when rest is followed by targeted mobility, strengthening, and movement retraining. |
| Do I need imaging? | Not always. Many people improve based on history and physical examination. Imaging may be considered when symptoms are severe, unusual, not improving, or when another diagnosis needs to be ruled out. |
| Can walking help? | Often, yes. Gentle walking can be useful if it doesn't ramp up symptoms. Many people tolerate walking better than sitting, but the right dose matters. |
| How do I know when to get checked? | If the pain keeps returning, limits daily activity, or you can't tell whether it's coming from the hip or the back, it's worth getting evaluated by a physical therapist. |
If piriformis pain is making it hard to sit, move, exercise, or figure out whether the problem is really your hip or your back, a physical therapist can help you sort it out and build a plan that fits your body. You can learn more or connect with a clinician through Highbar Physical Therapy.