A new blind spot, flashes of light, or the feeling that part of the room disappears when you turn your head can be unsettling. Many people first assume the problem is in the eye itself. Sometimes it is. But when the eyes look structurally normal and vision still feels wrong, the issue may be higher up in the system, in the part of the brain that processes what you see.
That area is the occipital lobe. When it's working well, you don't notice it. You read, track motion, find a doorway, recognize a face, and move through space. When it's injured, those everyday tasks can become slow, tiring, and surprisingly difficult.
As a neurorehabilitation clinician, I've seen how frustrating this can be for patients. The hardest part is often that the symptoms are real, but they don't always look obvious to other people. A person may walk into a wall on one side, lose their place while reading, or feel off balance in busy environments, even though standard eye structure looks fine.
The good news is that there are practical next steps. Understanding the anatomy helps. Knowing the common causes helps more. But the most useful question is usually this: What do I do now? That's where physical therapy and neurovisual rehabilitation matter.
Your Brain's Vision Center The Occipital Lobe
The occipital lobe sits at the back of the brain and serves as the brain's main visual-processing center. If your symptoms started after a stroke, concussion, head injury, migraine episode, or another neurological event, that location matters. Your eyes collect visual information, but your brain gives that information meaning.
A patient might say, “I can see something there, but I can't make sense of it fast enough.” Another might describe missing food on one side of the plate or losing half a line while reading. Those complaints often sound strange until you connect them to brain-based visual processing.
The occipital lobe is where incoming visual signals first reach the cortex for organized processing. When that system is disrupted, the result isn't always total blindness. More often, it's a mismatch between what the eyes take in and what the brain can interpret efficiently.
Practical rule: If vision changed suddenly, especially with headache, weakness, confusion, speech changes, or balance problems, seek urgent medical care first. Rehabilitation matters, but acute neurological symptoms need immediate evaluation.
In rehab, the goal isn't just to name the injured area. It's to identify how the visual problem affects walking, reading, driving decisions, balance, work, and daily safety. That's the difference between a general brain anatomy lesson and a useful recovery plan.
Anatomy of the Occipital Lobe
Think of the occipital lobe as a visual command center placed at the back of the brain. It is the smallest of the four major cerebral lobes and sits at the posterior of the brain, directly beneath the occipital bone. It typically accounts for about 10% to 18% of total brain volume, and it contains the primary visual cortex, or V1, the first major cortical relay for visual input, as described by the Cleveland Clinic overview of the occipital lobe.

Where it sits and why that matters
Its location at the back of the head is clinically useful. After a fall, a blow to the back of the skull, or a stroke affecting the posterior brain, visual symptoms make anatomical sense. The issue may not be the eyeball, retina, or lens. The issue may be the brain's ability to process the image after the eyes have already captured it.
This is why someone can have a normal-looking eye exam yet still report major visual dysfunction. The hardware at the front end may be intact. The processing center may not be.
For readers who want a broader visual map of the brain's major regions, the Orange Neurosciences brain guide is a helpful plain-language reference.
The key structures inside the occipital lobe
The best-known structure here is V1, also called Brodmann area 17. This is the first cortical stop for visual information. It handles the early breakdown of what you're seeing, such as edges, contrast, and basic spatial arrangement.
Behind the scenes, nearby visual areas build on that first pass. These regions don't just register that something exists. They help the brain sort out what the object is, where it is, and whether it's moving.
The occipital lobe doesn't work alone. It starts the cortical side of vision, then hands information off to wider brain networks that support recognition, attention, and movement.
That handoff is why occipital lobe injury can affect more than “seeing.” It can change navigation, reading speed, postural confidence, and how safe a person feels in a crowded setting.
How We Process and Interpret the Visual World
Vision happens in stages. Light reaches the eyes, the retina converts it into signals, and those signals travel deeper into the brain. The occipital lobe handles the first major cortical step of that process. According to StatPearls on occipital lobe anatomy and function, retinal input is relayed to V1 for initial feature extraction, then distributed to association cortex in Brodmann areas 18 and 19 for higher-order interpretation of color, form, motion, object recognition, and visuospatial analysis.
First the brain extracts basic features
The first pass through the visual cortex is fast and efficient. The brain identifies lines, contrast, orientation, and simple visual patterns. It's not deciding the full meaning of a scene yet. It's collecting the building blocks.
That distinction matters in rehab. A patient may technically “see” but still struggle with interpretation. When someone says, “My eyes work, but busy spaces overwhelm me,” that often reflects a processing problem, not a motivation problem.
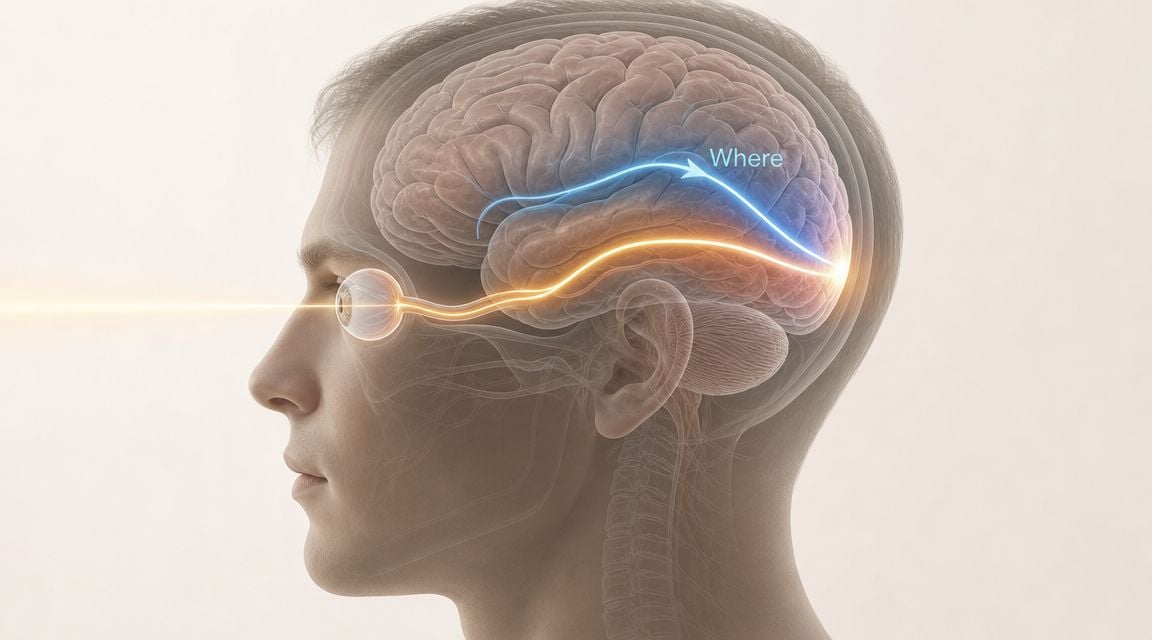
Then the brain answers two different questions
After the first cortical relay, visual information is distributed across broader networks. Clinically, it helps to think in two tracks:
- The what pathway helps identify form, color, and object details. That's what lets you recognize a coffee mug, a stop sign, or a familiar face.
- The where pathway helps track motion and spatial location. That's what lets you judge where a curb is, notice a person approaching from the side, or reach accurately for a doorknob.
A simple example is catching sight of a friend across a parking lot. One system helps you recognize that it's your friend. Another helps you judge where they are moving and whether you need to change your own path to meet them.
Why symptoms can feel oddly specific
This layered system explains why occipital lobe injuries can produce selective problems. A person may lose part of the visual field, struggle with motion-rich environments, or have trouble organizing visual clutter while still reading large single words. Another person may tolerate a quiet room but become dizzy and disoriented in a grocery store.
In physical therapy, these details guide treatment. We don't just ask, “Can you see?” We ask:
- What environments trigger symptoms
- Which side gets missed
- Whether reading, walking, or balance breaks down first
- How fatigue changes visual performance
Those answers tell us whether the priority is scanning, eye movement control, balance under visual challenge, or compensatory strategies for daily tasks.
Common Conditions Affecting Visual Processing
The occipital lobe can be disrupted in several different ways. The mechanism matters because it shapes both the symptom pattern and the rehabilitation plan. In practice, four groups come up often.
Stroke
A stroke can interrupt blood flow to tissue in the posterior brain or cause bleeding that affects visual-processing areas. When the occipital lobe is involved, the person may develop visual field loss or difficulty interpreting visual information even though the eyes themselves remain structurally intact.
Clinically, stroke-related occipital deficits are often abrupt. A patient may wake up unable to see one side of the visual world or suddenly lose the ability to read normally. In those cases, rehab usually focuses on safety, compensation, and retraining function around a more fixed visual change.
Traumatic brain injury and concussion
A blow to the head can disturb the visual system without creating the same pattern seen in stroke. Some patients have direct posterior impact. Others develop broader visual processing and oculomotor problems because the brain's visual networks are strained after injury.
Concussion-related symptoms often include motion sensitivity, eye strain, dizziness, trouble focusing, and overload in visually busy environments. For readers dealing with those issues, Highbar's concussion management service gives a useful overview of how rehab can address the functional fallout.
Brain tumors and post-surgical change
Masses in or near the occipital region can compress tissue, alter signaling, or require surgery that changes how visual information is processed. In these cases, symptoms may develop more gradually than in stroke. A patient may notice increasing reading problems, more collisions on one side, or unusual visual distortions before they understand the reason.
Rehabilitation in this group often has to account for fatigue, medication effects, and other neurological changes happening at the same time.
Migraine with aura
Migraine aura can create temporary visual symptoms that feel dramatic. People may describe flashing lights, zigzag patterns, shimmering areas, or blind spots. These symptoms don't necessarily mean permanent occipital injury, but they do reflect altered visual processing within brain networks that include the posterior cortex.
A temporary visual disturbance still deserves attention if it's new, severe, or different from your usual pattern. New neurological symptoms need medical clarification before anyone assumes “it's just a migraine.”
The key difference across these conditions is not merely cause. It's whether the problem is stable, fluctuating, progressive, or tied to exertion and sensory load. That distinction changes everything about treatment.
Signs and Symptoms of Occipital Lobe Damage
Patients rarely walk into clinic saying, “I think I injured my occipital lobe.” They describe lived problems. They miss objects on one side. They lose their place while reading. They feel unsafe on stairs. They say bright light or moving crowds make them feel disoriented.
That's why symptom language matters. The complaint often sounds functional before it sounds neurological.
What these symptoms can feel like
Some people develop visual field loss, often described as part of the world going missing. They may leave food on one side of the plate, ignore text on one half of a page, or bump into furniture on the same side repeatedly.
Others experience visual distortion rather than a clean field cut. They may report flashing lights, blurred patches, trouble judging motion, or the sense that the eyes can't keep up with the environment. In concussion and migraine, light sensitivity and visual overload are common complaints.
More complex symptoms can involve recognition. A person may see an object but need extra time to identify it. In higher-demand situations, face recognition, visual search, and spatial organization can become much less efficient.
Common Occipital Lobe Conditions and Associated Symptoms
| Condition | Common Visual Symptoms |
|---|---|
| Stroke affecting posterior brain regions | Visual field loss, missing one side of space, reading difficulty, bumping into objects |
| Concussion or mild traumatic brain injury | Light sensitivity, eye strain, dizziness with visual motion, trouble focusing in busy environments |
| Brain tumor or post-surgical change | Progressive visual changes, reading difficulty, spatial disorientation, trouble navigating |
| Migraine with aura | Flashing lights, shimmering patterns, temporary blind spots, visual distortion |
A related issue is headache. Visual strain, sensory overload, and post-concussion symptoms often travel together. If headaches are part of the picture, Highbar's guide to physical therapy and headaches can help patients understand how neck, vestibular, and visual factors may overlap.
Red flags that need prompt attention
Some symptoms should not be watched casually at home.
- Sudden visual change: New field loss, sudden darkness, or rapid onset of severe distortion warrants urgent medical evaluation.
- Neurological overlap: Vision change plus weakness, numbness, trouble speaking, severe headache, or confusion raises concern for stroke or another acute neurological event.
- Progressive decline: Symptoms that steadily worsen over days or weeks need medical workup, not just self-management.
If the visual complaint is changing quickly, rehabilitation is not the first step. Medical diagnosis is.
Once the cause is identified and medically stabilized, rehab can become much more specific and useful.
Diagnostic Process and Medical Treatments
The diagnostic process usually starts with a careful history and neurological exam. Clinicians want to know what changed, how quickly it changed, whether symptoms are constant or triggered, and whether the problem affects one side of the visual world, reading, balance, or all of the above.
What clinicians look for first
At bedside or in clinic, providers often screen:
- Visual fields: Can the person detect movement or targets on both sides?
- Eye movements: Do the eyes track smoothly and shift accurately?
- Functional behavior: Does the person miss obstacles, turn the head excessively, or lose place while reading?
- Neurological signs: Are there speech, sensory, coordination, or strength changes that point to a broader brain event?
Those observations help determine whether the problem is likely ocular, cortical, vestibular, or mixed.
Tests that clarify the picture
Formal visual field testing, often called perimetry, maps what parts of space the patient detects reliably. That's especially useful when someone reports a field cut but can't describe it clearly.
MRI and CT are commonly used to identify stroke, bleeding, structural lesions, swelling, or trauma-related change. For readers who want a plain-language overview of why CT may be used after head trauma, this article on traumatic brain injury CT scans gives a useful nontechnical summary.
Medical treatment usually targets the cause, not just the symptom. A stroke workup may focus on vascular management. A concussion plan may emphasize graded recovery and symptom monitoring. Tumor-related care may involve surgery, medication, or oncology treatment. Migraine care may focus on trigger management and medical prevention.
That's an important point for patients. Medical care stabilizes the condition and treats the disease process. Rehabilitation addresses what the condition has changed in daily life.
How Physical Therapy Helps Reclaim Your Vision
Once the medical issue is identified and the patient is stable, the next question is practical. How do you move through the world safely and efficiently if visual processing has changed?
Physical therapy offers significant value. A good neurorehabilitation plan doesn't try to promise a miracle. It identifies what's impaired, what's adaptable, and what strategies improve function. Recovery from visual field loss is often incomplete, but targeted rehabilitation can improve visual function and daily activities, with functional compensation tending to be more consistently successful than full field restoration, as summarized in this discussion of a 2025 systematic review on post-stroke visual field loss rehabilitation in the linked review summary.

What physical therapy can target
Physical therapists don't treat the occipital lobe in isolation. We treat the movement and function problems that happen when visual processing changes. That often includes:
- Visual scanning: Training the patient to systematically search into the missed side rather than waiting to notice it accidentally.
- Eye movement control: Working on saccades and smooth pursuits when reading, target finding, or visual tracking is inefficient.
- Balance under visual demand: Challenging postural control when the environment is busy, moving, or visually complex.
- Gait safety: Practicing walking, turning, obstacle negotiation, and stair use when field loss or motion sensitivity increases fall risk.
- Habituation and sensory tolerance: Gradually building tolerance to visual motion or environmental complexity when symptoms are triggered by stores, traffic, or screens.
For patients with dizziness, motion sensitivity, or visually induced imbalance, Highbar's dizziness and vertigo service describes how vestibular rehab often overlaps with visual rehabilitation.
What works better than vague advice
Patients are often told to “be careful” or “give it time.” Neither is a treatment plan. In practice, useful rehab is specific.
A patient with a left visual field cut may practice structured leftward scanning during walking, reading, and object search. A patient with post-concussion visual intolerance may start with short, controlled tracking work and simple balance tasks, then progress to more visually complex environments. A patient who loses place while reading may work on line tracking strategies, page anchors, and eye movement drills tied to actual reading goals.
Here are the interventions that tend to be clinically useful:
Task-specific scanning practice
This works best when it's tied to real activities. Finding items on a countertop, scanning shelves, locating signs in a hallway, and crossing a room safely are more meaningful than abstract drills alone.Oculomotor retraining
Saccades help the eyes jump accurately from one target to another. Smooth pursuits help track moving targets. If those systems are inefficient, reading and navigation often suffer.Balance and gait progression
Visual loss changes posture and confidence. Many people start moving more slowly, stiffly, or with an exaggerated head turn. Therapy can retrain safer movement patterns without reinforcing fear.Environmental modification
Sometimes the best first intervention is not an exercise. It's changing lighting, reducing visual clutter, improving contrast, or placing important objects in a more predictable location.
What doesn't work well
Some approaches fail because they aren't matched to the problem. Generic strengthening won't solve a visual field cut. Endless rest won't retrain scanning. Random online eye drills often create fatigue without improving function because they lack progression, task relevance, or clinical reasoning.
Another common mistake is chasing perfect restoration when compensation is the more realistic path. That doesn't mean giving up. It means focusing on the gains that matter most: safer walking, better reading efficiency, fewer collisions, less dizziness, and more independence.
The strongest rehab plans are honest. They aim for meaningful function first, not false certainty.
How therapists set goals that matter
In neurovisual rehab, goals should sound like life, not like a worksheet.
Examples include:
- Reading without losing the line
- Walking through a grocery store without veering or panic
- Finding the bathroom door in a busy hallway
- Navigating stairs safely
- Tolerating screen use long enough for work tasks
- Returning to exercise without symptom spikes
That's also why home programs have to be precise. I'd rather give a patient a short set of well-targeted drills they'll perform consistently than a long packet they won't use. The right dosage depends on fatigue, symptom irritability, and safety.
The role of adaptation
Many patients ask whether the brain can adapt. It can. But adaptation doesn't always look like the damaged function returning in full. Often it looks like better strategy use, faster scanning, improved confidence, smarter environmental setup, and stronger integration between vision, balance, and movement.
That's meaningful recovery. It's not cosmetic. It changes what a person can do.
Frequently Asked Questions About Recovery
Will my vision come back completely
Sometimes visual function improves, but complete return isn't guaranteed. In occipital lobe injury, recovery is often partial. The most reliable gains usually come from better compensation, scanning, and functional retraining rather than expecting the visual field to fully normalize.
How long does visual rehabilitation take
It depends on the cause, symptom severity, fatigue level, and the demands of your daily life. A person recovering from concussion may progress differently from someone with a stroke-related field cut. What matters most is whether treatment is targeted and whether daily function is improving.
Can physical therapy help with light sensitivity and dizziness after concussion
Yes, when those symptoms are linked to visual motion intolerance, vestibular dysfunction, or oculomotor strain. PT often addresses the overlap between eye movement control, balance, head motion, and sensory overload.
Is exercise good for brain recovery
In many cases, yes, as long as it's medically appropriate and dosed correctly. Aerobic activity can support recovery, mood, and tolerance to daily activity. If you're interested in the broader brain-side discussion, this article on brain health through lactate production offers a consumer-friendly overview of one reason exercise remains part of many neurorehab conversations.
If visual changes have affected your balance, reading, walking, or day-to-day confidence, working with a skilled rehab professional can help you build a plan that's specific to your symptoms and goals. Highbar Physical Therapy offers evidence-based care that helps patients improve function, move more safely, and regain independence after neurological and visual challenges.