Pain on the outside of your knee has a way of changing your plans fast. A run that felt smooth for the first couple of miles suddenly turns sharp on the downhill. A long walk becomes a limp on the way back. A bike ride that usually clears your head ends with one spot at the side of the knee getting more irritated with every pedal stroke.
For a lot of active adults, that pattern points to iliotibial band syndrome, often shortened to IT band syndrome or ITBS. The good news is that this problem is common, well understood, and very treatable. It usually does not mean your knee is damaged. It usually means your body is asking for a change in load, movement strategy, and strength.
That Sharp Pain on the Outside of Your Knee
The classic story goes like this. You feel fine when you start. Then, at a certain point, the outside of the knee starts to sting or burn. You try to push through it. The pain gets more specific, not less. Stairs bother it later. Sometimes sitting with the knee bent makes it ache too.
That pattern is frustrating, but it's also recognizable. Iliotibial band syndrome is the leading cause of lateral knee pain in runners and cyclists, with prevalence ranging from 5% to 14% of all running-related injuries, and it affects an estimated 1 in 7 to 1 in 20 long-distance runners, according to Johns Hopkins Medicine's overview of iliotibial band syndrome.
What it usually feels like
Patients often describe it in plain terms:
- Sharp at first: A pinpoint pain on the outer knee during activity
- Worse with repetition: More steps, more pedals, more hills, more irritation
- Annoying afterward: Soreness when walking, using stairs, or getting up after sitting
- Predictable: It often appears at a similar point in the workout
The location matters. Pain from the it band is usually very specific on the outside of the knee, not vague all over the joint.
What it does not mean
IT band pain can feel dramatic, but it usually isn't a sign that the knee is “wearing out” or that you've torn something major. In most cases, this is an overuse problem with a movement component. That distinction matters, because it changes what helps.
If your first instinct was to stretch harder, roll directly on the sore spot, or just stop all activity and hope it fades, you're not alone. A lot of people do that. It rarely solves the whole problem.
Understanding Your IT Band Anatomy and Function
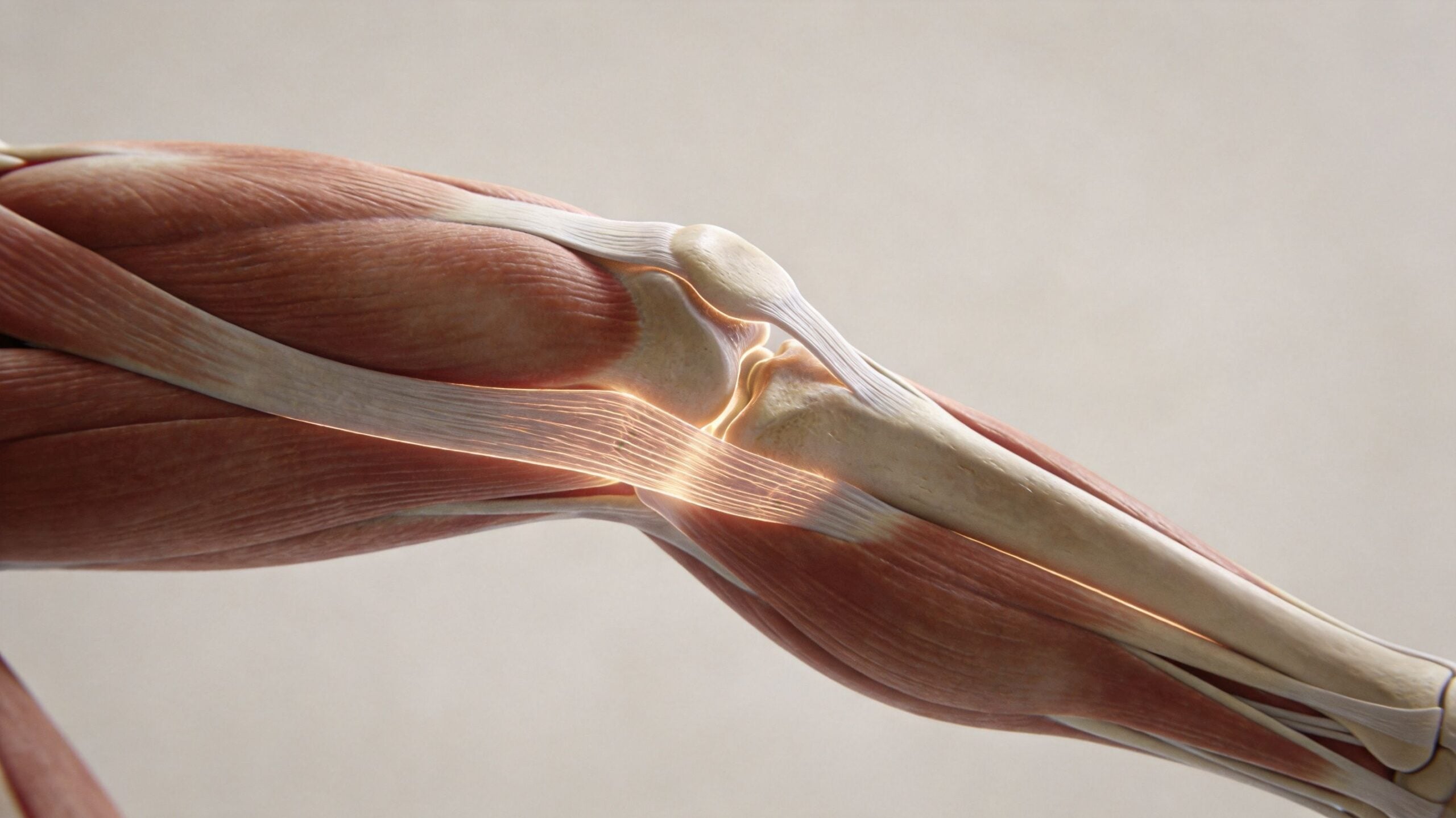
The iliotibial band isn't a muscle. It's a thick band of connective tissue that runs down the outside of the thigh from the hip toward the tibia below the knee. Think of it as a strong lateral support strap. It connects with muscles near the hip, especially the tensor fasciae latae and gluteus maximus, and helps manage load as you walk, run, climb, and change direction.
It stabilizes more than people realize
Your it band helps control the outside of the hip and knee during repeated single-leg loading. That's why symptoms often show up during running, hiking, and cycling. These activities ask the leg to accept force over and over while the pelvis and femur stay controlled.
If the hip muscles don't do their share, the it band often gets blamed because that's where the pain shows up. But the tissue itself is more of a load transmitter and stabilizer than a structure you can “loosen” on command.
For a deeper look at the hip side of the problem, see this guide to iliotibial band syndrome at the hip.
It also acts like an energy-saving structure
This aspect is often surprising. The it band isn't just there to hold things together. It also contributes to efficient movement. The human IT band can store 15 to 20 times more elastic energy per body mass than the similar structure in chimpanzees, and its energy-storage capacity is greater during running than walking, as described in Harvard's report on understanding the IT band.
That matters clinically. A healthy it band works as part of a spring-like system. It helps recycle force during gait. So when people say, “My it band is too tight, I need to stretch it out,” they're usually misunderstanding the tissue.
Clinical takeaway: The it band is built to handle tension. Rehab works best when it restores load sharing and movement control, not when it tries to force length into a structure that isn't designed to behave like a hamstring.
The Real Causes of IT Band Syndrome
For years, people were told their it band was “rubbing” back and forth over the outside of the knee like a rope over a corner. That explanation stuck because it sounds intuitive. It's also outdated.

Anatomical research shows the IT band is firmly anchored to the distal femur, which makes significant sliding or “friction” impossible. Instead, pain is caused by compression of a highly innervated fat pad between the IT band and the bone during knee flexion, based on this anatomical review in the British Journal of Sports Medicine.
Why that changes treatment
If the problem isn't friction, then “breaking up adhesions” by aggressively grinding on the band doesn't make much sense. The pain is better understood as compression plus poor load management.
The next question is why that compression gets worse in some people. In clinic, the answer is usually a mix of movement pattern and training error.
Common drivers I look for
- Hip abductor weakness: When the gluteus medius doesn't control the pelvis well, the thigh tends to drift inward and the knee collapses into valgus.
- Poor single-leg control: You don't need obvious weakness to have poor control. Many active people are strong in the gym but unstable when landing, stepping down, or running.
- Sudden load changes: More mileage, more hills, more speed work, more descents, more time on the bike, or a return after time off.
- Surface and route issues: Cambered roads, repeated one-sided turns, and long downhills can all irritate the same lateral structures.
- Sedentary patterns between workouts: Long hours sitting can leave the front of the hip stiff and push the body toward compensations once you get active.
The painful spot is often the end result. The root cause is usually higher up the chain.
What works better than the old model
A better treatment strategy focuses on the parts that influence compression at the knee:
- Calm the irritated area enough to move better.
- Restore hip and trunk control so the femur doesn't keep drifting inward.
- Reload gradually so the tissue can tolerate real activity again.
- Adjust the movement that triggered it, whether that's stride pattern, cycling setup, hill volume, or single-leg mechanics.
That's why many people fail when they only chase symptoms. They ice, stretch, or foam roll the sore spot, then return to the same loading pattern that caused the problem.
Effective Self-Care for Immediate Pain Relief
The first job is to settle things down enough that you can move without provoking the knee every few hours. Self-care can help. It just needs to be directed at the right target.

Stop trying to smash the band itself
Rolling directly on the outer thigh often feels productive because it's intense. That doesn't mean it's useful. The it band is dense connective tissue. You're not meaningfully lengthening it with a roller, and pushing hard on an already irritated lateral knee can make people more guarded, not less.
A smarter approach is to work on the muscles that feed tension into the system, especially the tensor fasciae latae, glutes, and lateral thigh musculature. If you want general guidance on choosing and using rollers, this article on foam rollers and their benefits is a helpful companion.
What to do in the first few days
Try this simple approach:
- Relative rest: Reduce or pause the activity that clearly triggers pain. This doesn't mean total bed rest. It means backing off enough to stop flaring it repeatedly.
- Ice after aggravating activity: Use it for comfort if the outer knee feels hot, sharp, or reactive afterward.
- Modify your route or workout: Skip hills, speed work, long descents, and deep stair volume for now.
- Foam roll nearby tissues: Target the upper outer hip, front-lateral hip, and glute region instead of driving pressure into the sore knee area.
- Gentle mobility: Easy hip mobility and light walking can be better than complete inactivity if they don't reproduce the sharp pain.
Practical rule: If a self-care technique makes the outside of the knee more irritated for the rest of the day, it's too aggressive for this stage.
What not to do
People usually get stuck because they keep repeating one of these mistakes:
- Don't chase pain with harder stretching. A stronger stretch isn't the same thing as better treatment.
- Don't test the knee every day with the same failing workout. Repeating the exact trigger delays recovery.
- Don't confuse sweating with progress. During an it band flare, the best session is the one that calms the knee and preserves good movement.
Self-care should create a window for strengthening. If it doesn't, it's incomplete.
A Phased Rehab Plan to Rebuild Strength
Rest alone rarely solves recurring it band pain. Symptoms may settle, but the movement pattern that overloaded the lateral knee often remains. A good rehab plan rebuilds capacity in stages.
Phase 1 goals
Early rehab is about reducing irritability and waking up the muscles that should be helping more.
Focus on low-load work that improves glute activation and pelvic control without provoking the knee. Good examples include side-lying clamshells, bridges, controlled side-lying hip abduction, and short bouts of single-leg balance near a wall or counter.
The standard here is control, not fatigue. If you feel the front of the hip doing all the work or the pelvis rolling backward, scale it down.
Phase 2 goals
Once day-to-day pain is calmer, the next step is building strength where many people are underpowered: the lateral hip, posterior hip, and trunk. The rehab then starts to look more like training.
Useful options include lateral band walks, bridge progressions, side planks, step-down variations, and split-stance loading done with good alignment. The goal is to keep the pelvis level and the knee tracking cleanly over the foot.
Get strong in positions that look like your sport. A runner needs control on one leg. A hiker needs control when lowering. A cyclist needs control through repeated flexion without drifting into compensation.
Phase 3 goals
The final phase ties strength back to function. You're preparing for impact, repetition, and confidence.
That means single-leg squats to a box, controlled lunges, hop preparation, return-to-run progressions, and terrain-specific practice if hills or hiking were part of the original problem. At this point, movement quality still matters more than volume.
3-Phase IT Band Rehab Protocol
| Phase | Goal | Example Exercises |
|---|---|---|
| Phase 1 | Reduce pain and restore muscle activation | Clamshells, bridges, side-lying hip abduction, supported single-leg balance |
| Phase 2 | Build hip and core strength with better control | Lateral band walks, side planks, step-downs, split-stance strength work |
| Phase 3 | Return to functional loading and sport-specific movement | Single-leg squats, lunges, hop preparation, graded return to running or riding |
How to progress without guessing
Use a simple filter before moving forward:
- Symptoms during exercise stay manageable. Mild awareness can be okay. Sharp lateral knee pain is not.
- Symptoms settle quickly afterward. If the knee stays angry into the next day, the dose was too high.
- Form holds up under fatigue. If the knee dives inward or the pelvis drops late in the set, you've found your limit.
This is also where people tend to rush. They feel better and jump back to their old mileage, long rides, or steep hikes before they've rebuilt the capacity to tolerate them. That's the cycle that keeps it band pain hanging around.
A note on exercise selection
You do not need a huge menu. You need a few exercises done well, progressed on purpose. A small program built around glute activation, frontal plane hip strength, single-leg control, and gradual return to load often works better than a long list of random stretches.
If your pain is stubborn, a physical therapist can fine-tune the dose, check your mechanics, and help decide whether the limiter is strength, control, mobility, training volume, or all of the above.
How to Prevent IT Band Syndrome from Returning
Once the knee settles down, prevention becomes less about “maintenance tricks” and more about keeping the whole system honest. The same mechanics that helped you recover are the mechanics that keep symptoms from coming back.
Keep strength work in your routine
If you've had it band pain before, hip and trunk work shouldn't disappear the moment you feel normal again. Most recurrences happen when people return to activity and stop the strength work that made them stable.
A simple plan works well:
- Before activity: Dynamic warm-up, a few activation drills, and a short build-up
- During the week: Regular glute and single-leg strength work
- During training cycles: Watch hill volume, downhill exposure, and sudden spikes in load
For broader training habits that reduce overuse problems, this guide on how to prevent running injuries is worth reading.
Use cadence and load to your advantage
For runners, one of the most practical adjustments is cadence. For athletes, especially those over 40, maintaining a running cadence above 170 steps per minute has been shown to reduce the risk of ITBS recurrence, according to this review on running-related factors and recurrence risk.
A slightly quicker cadence often shortens overstriding, reduces braking forces, and makes it easier to keep the leg landing under the body. It's not a magic fix, but it can be a useful tool when paired with strength and load management.
Watch the common relapse points
Most flare-ups happen after one of these changes:
- Training spike: A fast jump in volume, intensity, or elevation
- Form drift: Fatigue sets in and the knee starts collapsing inward again
- One-mode training: Running only, riding only, or repeating the same route without variation
- Ignoring early warnings: Tightness at the outer knee that appears for days before a full flare
Prevention is rarely about one stretch or one gadget. It's about keeping your mechanics and training load from drifting in the wrong direction.
If you hike, cycle, or play field sports, the same rule applies. Build capacity first, then add intensity.
When to See a Physical Therapist for Your IT Band
Self-care works well for mild cases, especially when you catch symptoms early and change load quickly. But some cases need a more precise plan.
Signs it's time to get help
Consider seeing a PT if:
- Pain keeps returning every time you resume activity
- Daily tasks hurt, including stairs, walking, or getting up from a chair
- You're not sure it's really the it band, and you want to rule out other knee or hip problems
- Your form changes because of pain, and you're starting to limp or compensate
- You've tried rest and basic exercises, but progress stalls
What a PT adds
A physical therapist doesn't just hand out generic stretches. A good exam looks at where the problem starts. That often includes single-leg control, hip strength, trunk stability, training history, and movement analysis during tasks that reproduce symptoms.
In practical terms, that can include hands-on work for the lateral hip and surrounding tissues, a targeted strength progression, and gait or activity analysis to identify why the knee keeps getting overloaded. If your sport includes cutting and deceleration, resources like these football injury prevention tips can also be useful for thinking about warm-up, movement quality, and lower-body resilience in a broader way.
For people who want formal guidance, Highbar Physical Therapy offers outpatient evaluation, exercise-based rehab, and telehealth support as one option among many PT services.
The main point is simple. If pain keeps cycling back, you probably don't need more willpower. You need a better mechanical answer.
If your it band pain isn't improving, or it keeps coming back when you return to running, cycling, hiking, or gym work, a physical therapist can help identify the underlying driver and build a plan that fits your activity level. Find a PT at Highbar Physical Therapy.
