If you're reading this with a sore upper arm, a fresh fracture diagnosis, or a shoulder that still doesn't feel right months later, the humerus suddenly feels a lot less like a textbook bone and a lot more like the center of your day. Reaching a shelf, pushing up from a chair, pulling on a shirt, and even letting your arm hang comfortably all depend on it.
For patients, the humerus is the long bone between the shoulder and elbow. For a new PT grad, it's also a mechanical bridge that has to coordinate with the scapula, rotator cuff, elbow, and forearm without much margin for error. When it gets injured, recovery isn't just about bone healing. It's about restoring motion, confidence, load tolerance, and clean movement patterns.
Anatomy of the Humerus Your Arm's Foundation
A patient with a humerus injury usually points to one sore spot. The exam rarely stays that simple. I may be screening shoulder motion, checking elbow alignment, testing sensation over the lateral shoulder, and watching how the scapula moves, because the humerus is the load-bearing link between both joints.
The humerus is the long bone of the upper arm. Its shape changes from top to bottom because its jobs change. Proximally, it needs mobility so the hand can reach space. Distally, it needs precision so the elbow and forearm can position the hand under load.

The proximal humerus and shoulder mechanics
At the top sits the humeral head, the ball of the glenohumeral joint. It articulates with the glenoid and contributes to flexion, extension, abduction, adduction, and internal and external rotation. That range is useful, but it comes with a trade-off. The shoulder gets freedom by relying heavily on soft-tissue control rather than bony constraint.
Just below the head are the greater and lesser tubercles, where the rotator cuff attaches. The greater tubercle accepts supraspinatus, infraspinatus, and teres minor. The lesser tubercle accepts subscapularis. In practice, these attachment points matter because even a small injury here can change how well the cuff centers the humeral head during elevation. A patient may say, "I can move it a little, but it feels wrong." That usually reflects mechanics, not just pain.
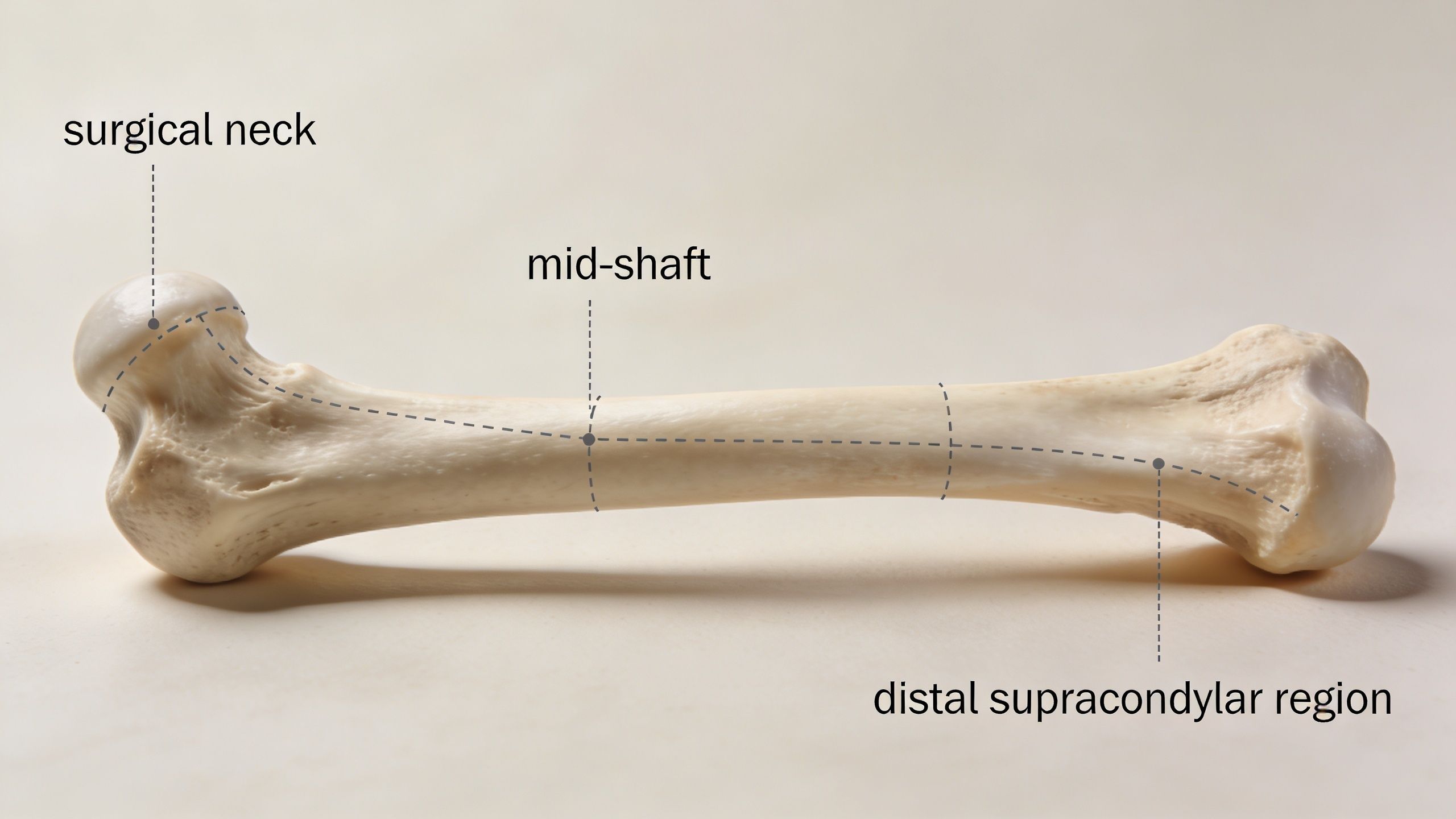
The surgical neck sits below the tubercles and deserves close attention after trauma. It is a common fracture region, and the axillary nerve travels nearby, as outlined in proximal humerus anatomy details.
Clinical point: After a proximal humerus injury, inability to actively lift the arm can reflect pain, rotator cuff dysfunction, joint stiffness, or nerve involvement. Good rehab starts by sorting out which problem is actually driving the loss.
The shaft and the distal humerus
The shaft is the central lever arm of the upper limb. It gives the shoulder and elbow a stable connection so force can travel cleanly from the trunk to the hand. When the shaft is fractured or badly deconditioned after immobilization, patients often notice this during ordinary tasks first. Reaching for a seatbelt, carrying groceries, pushing open a door, and catching themselves during a stumble all feel weaker and less coordinated.
Along the shaft, surface landmarks also matter clinically. The deltoid tuberosity marks the insertion of the deltoid, and the radial groove is closely related to the radial nerve. That relationship helps explain why a mid-shaft injury can affect wrist and finger extension as well as arm pain.
At the distal end, the bone becomes more specialized. The trochlea articulates with the ulna, and the capitulum articulates with the radial head. Together they let the elbow flex and extend while also supporting forearm rotation through the radiocapitellar relationship. The medial and lateral epicondyles serve as attachment sites for the forearm flexor and extensor groups, which is why local tenderness here can reflect tendon overload even when the original problem started higher up the chain.
The olecranon fossa accommodates the ulna during terminal extension, helping guide end-range elbow motion, as described in distal humerus elbow mechanics). If that region is irritated, stiff, or blocked by swelling after injury, patients often feel a hard stop when trying to fully straighten the arm.
For patients, the humerus works like a shaped strut between a very mobile shoulder and a very task-specific elbow. For a new PT grad, that is the key clinical lens. The bony anatomy explains where force travels, which tissues are stressed, and why rehabilitation has to progress from protection to motion to strength to full function rather than jumping straight to exercises.
Common Humerus Injuries and Conditions
The humerus typically comes to mind only when it breaks, and fractures are the main reason this bone gets urgent attention. They matter because location changes everything: the likely mechanism, the structures at risk, and the rehab strategy.
Humerus fractures account for 5-20% of all fractures, and the surgical neck is the most common fracture site at 50-60% of cases. These injuries are often seen in adults over 50 after a low-energy fall. Up to 80% of proximal humerus fractures are minimally displaced and may be treated non-surgically, while axillary nerve injury occurs in 10-20% of proximal fractures (humerus fracture patterns and management).
Proximal fractures
A proximal humerus fracture usually disrupts shoulder function first. Patients often guard the arm tightly against the body and struggle with basic movements like reaching the face or washing hair.
In older adults, low bone density changes the injury story. A simple fall can produce a fracture that looks dramatic on an X-ray but still behaves well with a sling and careful progression. In younger adults, high-force trauma raises more concern about displacement, associated soft tissue injury, and tolerance for delayed mobility.
Shaft fractures and nerve concerns
Mid-shaft injuries behave differently. The shoulder may still move somewhat, but the arm loses its stable beam. Patients describe a deep ache, pain with any jarring, and a strong sense that the arm is unreliable.
For clinicians, the neuro exam is critical. The humeral shaft sits close to important neural structures, and a fracture here should prompt careful screening of wrist and finger extension, grip changes, and altered sensation. What works well is repeated reassessment, not a single nerve screen on day one.
A patient can look mechanically improved before the nervous system has fully settled. Keep checking.
Distal injuries and related conditions
Distal humerus fractures are closer to the elbow and tend to create a different presentation: swelling, pain with bending or straightening, and a clear block to functional tasks like pushing, lifting, or turning a doorknob.
Other conditions involve the humerus even when the bone itself isn't broken:
- Shoulder dislocation: The humeral head slips out of its normal position, often leaving the shoulder unstable and guarded afterward.
- Tuberosity injury: The bony anchor for cuff tissue can become painful or displaced, especially after trauma.
- Post-traumatic stiffness: The bone may heal, but the shoulder and elbow don't automatically recover normal motion.
- Malunion or nonunion: Alignment or healing problems change mechanics and often leave patients weak or stiff even after the acute phase.
What doesn't work is treating every humerus injury as “just a shoulder problem” or “just an elbow problem.” The bone links both ends. A good exam always looks above and below the pain site.
Signs Symptoms and Clinical Diagnosis
A humerus injury usually announces itself quickly. Patients often report immediate pain, swelling, bruising, and a sharp drop in function. Some hear or feel a pop. Others know the arm doesn't move normally anymore.
The exam starts before anyone touches the arm. Posture, swelling, deformity, bruising pattern, guarding, and willingness to move all give useful information. Then the clinician checks tenderness, active motion if appropriate, and neurovascular status.
What usually sends someone for urgent evaluation
These signs deserve prompt medical attention:
- Severe pain after a fall or direct blow: Especially if the pain spikes with any attempt to lift or rotate the arm.
- Visible deformity or unusual contour: This may suggest fracture or dislocation.
- Rapid swelling and bruising: These don't confirm a fracture by themselves, but they raise concern.
- Loss of motion: Inability to bend the elbow, raise the arm, or use the hand normally matters.
- Numbness or weakness: Sensory change or motor loss raises the stakes and needs a careful nerve exam.
What the clinician is looking for
A focused physical exam checks whether the shoulder, shaft, or elbow is the main pain generator. Clinicians also look for a painful block to elbow motion. The olecranon fossa on the posterior humerus acts as a mechanical stop that prevents extension beyond 180 degrees, so pain or a block in that motion can point toward fracture or pathology in the distal humerus region, especially during an elbow exam.
Imaging confirms the diagnosis and shows alignment. X-rays usually answer the first question: Is there a fracture, and where is it? If the fracture pattern is complex, imaging helps the team decide whether protection alone is enough or whether the arm needs surgical stabilization.
When the story, exam, and imaging don't match, slow down. That mismatch often reveals the part of the injury that needs the most attention.
For patients, the main point is simple. If pain, swelling, and loss of function come on fast after trauma, don't try to “wait it out” for days.
Medical Treatments for Humerus Injuries
Once a humerus injury is identified, the treatment decision usually falls into two paths: protect it and let it heal, or stabilize it surgically because the position or pattern makes healing less predictable. The right answer depends on alignment, fragment position, tissue involvement, symptom behavior, and the person's functional needs.

Non-surgical care and when it fits
For many fractures, especially those with acceptable alignment and stable behavior, non-surgical management works well. That often means a sling or fracture support, pain control, and a staged plan for motion.
Expectations play a key role. Rest alone isn't the same as recovery. Protection helps the bone, but too much immobilization can stiffen the shoulder, elbow, wrist, and hand. Patients often understand this trade-off better if they've seen similar fracture decisions in other body regions, such as the practical comparison in this guide on splint vs cast for wrist fracture.
Surgical care and the decision points
Surgery enters the picture when fracture alignment is poor, stability is questionable, or the risk of healing in a bad position is too high. In proximal humerus injuries, radiographic criteria often guide that call. The Neer classification considers a fragment displaced if it is separated by more than 1 cm or angulated more than 45 degrees, and those features increase concern for malunion or nonunion and make surgical stabilization more likely (Neer criteria for proximal humerus fracture decisions).
Surgical options may include plates and screws or intramedullary fixation. What surgery does well is restore alignment and give a more secure framework for healing. What it doesn't do by itself is restore shoulder rhythm, cuff timing, elbow extension, or confidence using the arm.
Treatment trade-off: Surgery can improve mechanical stability. It also introduces surgical pain, scar management, and a different rehab progression.
There are also practical questions outside the clinic. Patients sometimes need to understand work restrictions, accident-related documentation, or the broader impact of a broken arm. In that context, some people find these insights into broken arm injury value useful for understanding how injury severity, treatment course, and recovery limitations may be viewed in a legal setting.
What works best is matching the medical plan to the fracture and then moving into rehab at the right pace. What doesn't work is assuming “non-surgical” means minor, or that “surgical” means the hard part is over.
The Role of Physical Therapy in Humerus Recovery
A common rehab moment looks like this: the follow-up X-ray is reassuring, but the patient still cannot wash their hair, reach a shelf, or lower the arm without a shrug. The bone may be healing on schedule. The arm is not yet functioning on schedule.
Physical therapy closes that gap between healing tissue and useful movement. After a humerus injury, people do not just lose strength. They lose timing, confidence, joint motion, and the normal coordination between the shoulder blade, humeral head, elbow, forearm, wrist, and hand. Immobilization protects the injury early, but it also creates stiffness, guarding, and compensatory patterns that can linger long after the fracture line starts to fade on imaging.
In clinic, I watch for the problems patients do not always notice themselves. The shoulder blade may hike instead of rotate well. The rotator cuff may fire late. Breathing gets shallow because the whole upper quarter feels guarded. The elbow stays slightly bent all day because that position feels safer. Those adaptations make sense early. They become obstacles later.
What physical therapy is trying to restore
Good rehab works on several targets at the same time:
- Pain and swelling control: less guarding, better tolerance for movement, and better sleep
- Range of motion: shoulder, elbow, forearm, wrist, and hand mobility all matter
- Muscle capacity: rotator cuff, deltoid, scapular stabilizers, biceps, triceps, grip, and postural muscles often lose ground quickly
- Movement quality: reducing shrugging, trunk lean, and other substitutions that hide weakness or stiffness
- Functional tolerance: getting back to dressing, driving, lifting, pushing, carrying, work tasks, and sport without flaring symptoms
That combination is why PT is more than a sheet of exercises. It includes hands-on cueing, dose control, symptom education, and regular changes based on healing stage, pain behavior, and the actual demands of the patient's day.
Why precision matters in rehab
As noted earlier in the anatomy discussion, the humerus has predictable proportions that influence how the shoulder and elbow move together. In practice, that means rehab goals should be based on the person's mechanics, not on a generic instruction to "stretch more" or "strengthen the shoulder."
If overhead motion is limited, the problem might be capsular stiffness. It might also be poor humeral head control, weak cuff support, limited thoracic extension, or scapular upward rotation that is out of sequence. Those are different problems, and they do not respond to the same exercise at the same time. For readers who want a practical example of later-stage shoulder loading, these rotator cuff strengthening exercises fit after pain is calmer and motion is good enough to train without compensation.
Most humerus rehab setbacks come from protection that lasts too long, not from one muscle or one joint failing by itself.
That point matters to both audiences reading this. New PT grads need to assess the whole movement pattern instead of chasing isolated deficits. Patients need to hear that stiffness and weakness after the bone starts healing are common, expected, and usually treatable with a structured plan that progresses at the right pace.
Phased Rehabilitation Protocol and Recovery Timelines
Recovery after a humerus injury works best when it follows tissue healing, not impatience. The timeline varies with fracture location, fixation, pain response, and surgeon guidance when surgery is involved. Still, most successful rehab follows the same broad logic: protect first, restore motion second, rebuild capacity third, and return to full function last.
The biggest mistake is doing too much too early. The second biggest mistake is doing too little for too long.
A practical progression
Early on, the arm needs support and gentle movement that doesn't threaten healing. As pain settles and medical clearance expands, the shoulder and elbow need more active work. Strengthening starts small, usually with low-load control before heavier resistance. Final-stage rehab should look like real life again, not endless basic drills.
Here's the framework I use most often in clinic.
| Phase | Typical Timeline | Primary Goals | Example Activities |
|---|---|---|---|
| Phase I Protection | Early healing period | Protect the fracture or repair, reduce pain and swelling, maintain safe motion in nearby joints | Sling management as prescribed, hand and wrist motion, gentle pendulums when cleared, posture work, supported elbow and forearm motion |
| Phase II Early mobility | After initial protection when cleared | Restore shoulder and elbow range without provoking instability | Table slides, wand-assisted motion, pulley work if appropriate, active-assisted flexion, gentle scapular setting |
| Phase III Early strengthening | Once motion is improving and load is tolerated | Build cuff, deltoid, scapular, and arm strength with clean mechanics | Isometrics, light band work, sidelying external rotation, supported reaching, controlled carrying tasks |
| Phase IV Return to function | Later recovery stage | Restore endurance, confidence, and task-specific capacity | Overhead progressions, closed-chain loading as appropriate, work simulation, sport-specific drills, lifting progressions |
What each phase feels like to the patient
Phase I is frustrating because it can feel passive. Patients want to “get back at it,” but this stage rewards patience. Good treatment here keeps the neck, hand, wrist, and scapula from getting stuck while respecting the healing site.
Phase II is where many people think they should be farther along than they are. Motion returns unevenly. Flexion may improve before rotation. Elbow extension may lag because the arm has been held in a guarded position. That's normal, but it still needs active work.
Rehab rule: If motion improves only when someone else moves the arm, the patient isn't ready to call that function.
Phase III is where mechanics matter most. This is the stage where shrugging, trunk lean, and elbow flare show up. Light resistance is useful, but only if the patient can control the path of motion. A few good reps beat a long set of sloppy ones every time.
Phase IV should resemble the patient's real goals. For one person, that's fastening a bra or carrying groceries. For another, it's pressing overhead, returning to throwing, or tolerating a full work shift.
Tools that help and mistakes that slow recovery
Rehab tools can support progress, but they shouldn't replace sound clinical reasoning. Bands, dowels, pulleys, grip trainers, and wall slides all have a place. In scarred or post-surgical cases, some clinics also consider modalities such as ultrasound for scar tissue when they fit the presentation, though exercise progression still drives the outcome.
Common setbacks usually come from one of these patterns:
- Protecting too long: The bone may be safer, but the shoulder and elbow get harder to recover.
- Advancing load too fast: Pain spikes, guarding returns, and confidence drops.
- Ignoring the scapula: The arm can't move well off an unstable base.
- Skipping distal work: Hand, wrist, and forearm stiffness can limit overall function.
- Training only range: Motion without strength and coordination doesn't hold up in daily life.
Patients often ask for an exact date when they'll feel normal. A better answer is this: recovery is usually a sequence, not a switch. Pain settles first, then motion improves, then strength returns, then the arm starts to feel like yours again.
Preventing Re-Injury and Finding Expert Care
The humerus usually gets injured during a specific event, but re-injury often comes from a pattern. Poor balance, rushed return to activity, persistent stiffness, incomplete strength recovery, and fear-based movement all raise the odds that the arm won't tolerate normal demands well.
For older adults, prevention often starts with the environment and with bone health conversations. Remove fall hazards at home, use stable footwear, and don't ignore a sudden drop in confidence with stairs or uneven ground. If a low-energy fall caused the fracture, that should prompt a broader conversation with your medical team about underlying contributors.
Prevention that actually translates to daily life
For active adults and athletes, prevention isn't just “strengthen the shoulder.” It usually means building shoulder capacity in context:
- Warm up with purpose: Prepare the cuff, scapular muscles, and trunk before overhead or contact activity.
- Earn end range: Don't force overhead motion if the shoulder still cheats with shrugging or trunk lean.
- Load gradually: Return to lifting, throwing, or manual work in steps, not in one jump.
- Keep the elbow and forearm in the program: A shoulder that moves well with a stiff elbow still won't function smoothly.
- Watch the compensations: Pain often drops before movement quality improves.
When it's time to see a PT
You don't need to wait until the arm feels hopeless. A PT evaluation makes sense when:
- Pain persists: The fracture may be healing, but the shoulder or elbow still limits sleep or daily function.
- Motion stalls: You can't reach, rotate, straighten, or bend the arm the way you need to.
- Strength hasn't come back: Carrying, pushing, pulling, or lifting still feels unreliable.
- You feel stuck after surgery or immobilization: That usually means the plan needs progression, not just more time.
- You're returning to work or sport: Higher-demand tasks need a more deliberate bridge.
Recovery is rarely linear. A short plateau doesn't mean failure. It usually means the program needs a more precise target.
The main takeaway is encouraging. A humerus injury can interrupt nearly everything you do with your arm, but individuals typically improve when the plan matches the stage of healing and the demands of real life. The bone has to heal. The shoulder and elbow have to move. The nervous system has to trust the arm again.
If you want help making sense of shoulder or arm pain, recovering after a fracture, or figuring out the next step in rehab, Highbar Physical Therapy offers physical therapy evaluation and treatment focused on restoring movement, strength, and confidence without unnecessary delay.