You slip on ice, throw a hand out to catch yourself, and feel pain shoot from your wrist up the forearm before you even hit the ground. A few minutes later, your wrist is swelling, you can't grip your phone normally, and every small movement feels wrong. That sequence is so common that many patients can describe it almost frame by frame.
The radius bone usually doesn't get much attention until it stops doing its job. Then suddenly you notice how often you rely on it. Turning a key. Twisting a doorknob. Carrying a grocery bag. Pushing up from a chair. Even rotating your palm to accept change or hold a bowl of soup depends on a forearm and wrist system working together.
As a physical therapist, I see the same misunderstanding over and over. People think they injured "the wrist," when the actual issue is often a fracture or malalignment involving the radius bone near the wrist. DPT students see the other side of that same problem. They may know the landmarks and fracture names, but not yet appreciate why a few degrees of stiffness in rotation can change a person's whole day.
A radius injury isn't just about a broken bone healing on an X-ray. It's about whether you get back your forearm rotation, your wrist mechanics, your grip, and your confidence using the arm. That's why treatment decisions matter early, and why rehab isn't a generic handout after the cast comes off.
Introduction A Moment on the Ice a Lifetime of Impact
A fall onto an outstretched hand seems simple. The body reacts fast, the hand hits first, and force travels straight into the wrist and forearm. In many cases, the radius bone takes that load.
For some people, the first sign is obvious deformity. For others, it's more subtle. The wrist swells quickly, the forearm aches, and they keep trying to "shake it off" until they realize they can't turn a doorknob or lift a coffee mug without sharp pain.
What makes this injury frustrating is how disruptive it is to ordinary life. You may still be able to walk, talk, and drive with one hand, so it doesn't always feel dramatic at first. But by the end of the day, simple tasks start piling up.
Practical rule: If pain, swelling, loss of grip, or visible shape change starts right after a fall onto the hand, assume it needs medical evaluation rather than waiting to see if it settles.
I explain the radius bone to patients as the forearm's working lever and rotating partner. When it's injured, the problem often shows up in places people don't expect. Wrist stiffness. Elbow discomfort. Weak grip. Trouble turning the palm up to hold a plate or down to type.
For clinicians in training, anatomy becomes functional reasoning. A fracture pattern matters, but so does the person's actual goal. An office worker may struggle with keyboard positioning. A parent may struggle with lifting a child. An athlete may have nearly full motion but still lack rotational control under load.
That difference matters because recovery isn't just about healing. It's about restoring the mechanics that let the whole upper limb move normally again.
Anatomy and Function of the Radius Bone
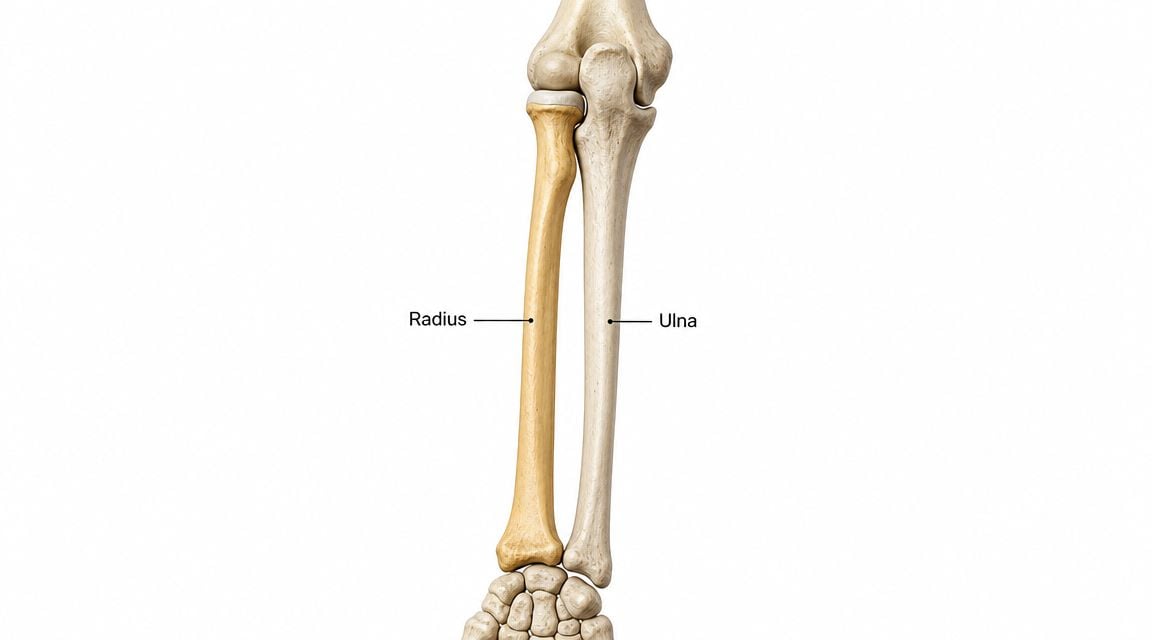
The radius is the forearm bone on the thumb side, and its job is more specialized than many patients expect. It does not just add structure. It helps place the hand where the task demands it, whether that means turning a key, catching a ball, pushing up from a chair, or carrying a pan with the palm up.
Why the radius bone matters so much
The radius works as the forearm's primary moving bone during rotation. It meets the humerus at the elbow, the ulna at both radioulnar joints, and the wrist bones at the hand end. That multi-joint role is why a radius injury can affect far more than one sore spot.
In practical terms, the radius helps you:
- Turn the palm up to hold a bowl, receive change, or wash your face
- Turn the palm down to type, use a mouse, or push through the hand
- Guide wrist motion during bending, straightening, and side-to-side movement
- Transmit load from the hand up the forearm during grip, lifting, and weight-bearing
This matters in rehab because bone healing alone is not the whole target. If rotation stays limited, patients often regain a "usable" arm but still struggle with the positions daily life calls for.
Key landmarks patients and students should know
At the elbow, the radial head helps the forearm rotate while also contributing to elbow mechanics. Along the shaft, the radius has a natural bow. That curve is not a minor detail. It helps the radius move efficiently around the ulna during pronation and supination. If that shape changes after a fracture, forearm rotation often pays the price.
Near the wrist, the radius broadens and forms much of the joint surface that accepts force from the hand. Clinically, this is why distal radius injuries can create problems with both comfort and control under load. A patient may say, "my wrist feels weak" or "it just doesn't track right." Often, they are describing a mechanical issue, not just pain.
For students, anatomy directly informs decision-making. A small loss of alignment at the distal radius may still let someone flex and extend the wrist reasonably well, yet leave them limited in pronation, supination, grip efficiency, or load tolerance. Those deficits change treatment choices. Early exercise selection, splint positioning, and progression of weight-bearing all need to protect healing tissue while preserving the motion that is hardest to get back.
The radius is the part of the forearm system that lets the hand arrive in the right position for the task. When that positioning system is off, everything downstream feels harder.
Common Radius Injuries and Their Symptoms
When individuals search for the radius bone, they're really dealing with an injury near the wrist. That makes sense. The distal radius is a common place to fracture after a fall, especially when the hand is out in front trying to absorb impact.

Injury patterns you'll hear about
Some names show up often in orthopedic conversations:
- Colles fracture. This usually refers to a distal radius fracture pattern associated with a fall on an outstretched hand, often with a visible wrist deformity.
- Smith fracture. This is commonly linked to a fall onto the back of the hand, creating a different displacement pattern.
- Radial head fracture. This happens closer to the elbow and often limits rotation and elbow comfort.
- Combined forearm injuries. When the radius and nearby structures lose alignment together, the mechanical problem becomes larger than a single break.
The key clinical point isn't memorizing names. It's matching the mechanism to the likely motion loss and stability problem.
Symptoms that deserve attention
The Physio-pedia overview of the radius notes that the radius's dual-joint role means radial fractures, especially distal fractures, can cause functional loss beyond the fracture site itself, including reduced rotation and altered wrist stability. That is exactly what patients report.
Common symptoms include:
- Immediate pain after a fall or direct impact
- Rapid swelling around the wrist or forearm
- Bruising that may spread over the next day
- Visible deformity or an abnormal wrist angle
- Weak grip or inability to hold everyday objects
- Pain with turning a key, jar lid, steering wheel, or doorknob
- Limited elbow or forearm motion if the injury is closer to the radial head
Some people also report tingling in the hand or fingers. That doesn't prove a nerve injury, but it raises concern for swelling or associated soft-tissue involvement and should be assessed promptly.
What symptoms often mislead people
A patient may still wiggle the fingers and assume nothing is broken. That isn't a reliable test. Many people with a distal radius fracture can move the hand a little, but they can't load it, rotate it, or tolerate pressure through the palm.
By contrast, a radial head fracture may not look dramatic at the wrist at all. The person mainly notices that they can't fully turn the forearm or straighten the elbow comfortably.
If someone says, "It hurts most when I try to rotate my palm," I pay close attention to the radius because that complaint often reflects more than a simple wrist sprain.
How Radius Fractures Are Diagnosed
Diagnosis starts with the story. A clinician wants to know how you fell, where you felt pain first, whether you heard a crack, and whether your symptoms changed quickly afterward. The mechanism often points toward the likely fracture location before any image is taken.
What the exam is checking
The physical exam looks for several things at once:
- Shape and swelling. Is there an obvious deformity or a rapidly enlarging area?
- Skin integrity. Is the fracture closed, or is there a wound that raises concern for an open injury?
- Circulation. Are the fingers warm, and does blood return normally after pressure?
- Sensation and movement. Can you feel touch normally, and can you move the fingers?
This isn't just routine. It helps identify urgent issues involving blood vessels, nerves, or severe displacement.
Why X-rays come first
For most suspected radius fractures, X-rays are the first imaging step. They help identify where the break is, whether the fragments are displaced, and whether the fracture appears to involve the joint.
Clinicians also look at alignment. In practice, that means they aren't only asking, "Is it broken?" They're asking whether the bone position is close enough to preserve future motion and function or whether it looks unstable.
A follow-up X-ray may also matter after reduction or during immobilization, because a fracture that starts in acceptable alignment can still shift.
When more imaging is needed
A CT scan may be ordered when the fracture pattern is complex or when the joint surface appears involved. That added detail can matter if the team needs to understand fragment position more precisely before deciding on surgery.
For patients, the practical takeaway is simple. More imaging doesn't always mean the injury is worse than expected. Sometimes it means the first X-ray showed enough complexity that the surgeon wants a clearer map before choosing treatment.
For students, the important habit is to connect imaging back to function. Joint involvement, displacement, and contour loss don't matter only because they look abnormal. They matter because they can block motion, change load transfer, and leave the patient with persistent stiffness if not addressed well.
Non-Surgical vs Surgical Fracture Management
A patient can fall, hear the word "fracture," and assume surgery is automatic. It often is not. The treatment decision usually comes down to a more practical question: can the radius heal in a position that preserves wrist motion, forearm rotation, and load transfer through the hand?

When non-surgical care makes sense
The AAFP guidance on common radius and ulna fractures supports nonoperative care for incomplete or minimally displaced fractures. It also notes that some displaced extra-articular distal radius fractures can be treated without surgery if the reduction is acceptable and stays that way during follow-up.
In clinic, that usually means the fracture can be lined up well enough without an incision, then held with immobilization while the bone consolidates. A typical sequence looks like this:
- Reduction if needed. The clinician restores alignment without opening the skin.
- Immobilization. A splint or cast protects that alignment during early healing.
- Repeat X-rays. The team checks whether the fracture is holding or drifting.
- Rehabilitation after immobilization. Motion and strength are restored once the bone is ready.
Patients often ask why the support changes over time. Swelling, fracture stability, and skin tolerance all matter. This guide on splint vs cast for wrist fracture explains why one option may fit better at one stage than another.
When surgery becomes the better option
Surgery is considered more often when the fracture is unstable, clearly displaced, involves the joint surface, or repeatedly loses position in a cast. The goal is not only to get the bone to unite. The goal is to restore the shape of the radius closely enough that the wrist and forearm still move the way they should months later.
That point matters more than many patients realize. A small change in alignment can create a much larger problem in function, especially for pronation and supination. If the radius heals shortened, tilted, or rotated, the person may later say, "My bone healed, but I still can't turn a doorknob well or carry a pan comfortably."
A common operation is open reduction and internal fixation (ORIF). The surgeon repositions the fragments and secures them with hardware such as plates and screws.
The trade-offs that actually matter
Both paths have benefits and costs. Good decision-making means matching the fracture pattern to the least burdensome option that still protects long-term function.
| Path | What it may avoid | What it may risk |
|---|---|---|
| Non-surgical management | Incision, hardware, and the demands of surgical recovery | Loss of alignment during healing, more time immobilized, and residual deformity if the fracture shifts |
| Surgical management | Better control of alignment in unstable patterns and earlier confidence in fracture position | Surgical pain, scar sensitivity, hardware irritation, and stiffness if postoperative motion is delayed or too aggressive |
For DPT students, the clinical reasoning point is this: alignment is not just an imaging issue. It predicts motion quality. In forearm fractures, restoring the normal contour of the radius matters because that shape helps the ulna and radius rotate around each other efficiently. In distal radius injuries, joint congruity matters for the same reason. Small articular or positional errors can become persistent limits in grip, weight-bearing tolerance, and forearm rotation.
A fracture can be healed on X-ray and still leave the arm mechanically underperforming. That is why treatment planning has to focus on future motion, not union alone.
Physical Therapy A Phased Approach to Recovery
Patients often expect rehab to begin after the cast comes off or after the incision closes. In reality, recovery starts much earlier. Physical therapy doesn't just chase motion at the end. It protects function all the way through the healing process.

Phase one protection and motion where it's safe
During immobilization, the fracture is the headline, but stiffness is already trying to build in the background. This stage usually focuses on pain control, swelling management, and keeping uninvolved areas moving.
Common priorities include:
- Finger mobility so the hand doesn't become puffy and stiff
- Shoulder and elbow movement within medical precautions
- Elevation and symptom management to limit swelling
- Education about safe hand use, sleeping position, and warning signs
This phase is where many patients make an early mistake. They either stop using the whole arm entirely, or they test the wrist too aggressively because the hand "feels a little better." Neither works well.
The radius also matters above the wrist. The radial tuberosity is the insertion for the biceps brachii, which makes the bone mechanically relevant to elbow flexion and powerful supination, as explained in TeachMeAnatomy's radius overview. That is why rehab has to consider the entire upper limb, not just the distal forearm.
Phase two early mobility after immobilization
Once the bone is sufficiently protected and the medical team clears motion, the next task is restoring range without provoking setback. The big targets are usually wrist flexion, wrist extension, forearm pronation, forearm supination, and hand use.
A typical early mobility session may include:
- Gentle wrist flexion and extension
- Supported forearm rotation with the elbow tucked in
- Radial and ulnar deviation in small, controlled ranges
- Tendon gliding and hand opening exercises
- Soft tissue and scar work when appropriate after surgery
If surgery was involved, scar mobility can become part of treatment. Patients often benefit from practical guidance on incision recovery and mobility work. Highbar's article on how to prevent scar tissue after surgery is a useful companion for that phase.
Early motion should feel purposeful, not forceful. If you crank hard into stiffness, the wrist often gets more guarded, not less.
For students, exercise selection demands clinical reasoning. A patient who lacks supination after a distal radius fracture may not need more generic wrist stretching. They may need precise cueing, protected rotational loading, and improved proximal control.
Phase three rebuilding strength and load tolerance
Motion alone isn't enough. Many patients can move the wrist reasonably well but still can't carry a pan, push through the hand, or open a tight jar.
This phase usually adds:
| Focus | Examples |
|---|---|
| Grip strength | stress ball squeezes, therapy putty, towel wringing |
| Wrist strength | light wrist curls, extension work, controlled deviation |
| Rotation strength | resisted pronation and supination with a hammer or light lever |
| Functional loading | table weight shifts, modified push support, carrying drills |
The progression matters more than the exercise list. If someone still has a reactive, swollen wrist, heavy loading is too early. If motion is nearly normal but confidence is low, functional carrying and task simulation may matter more than isolated strengthening.
This is also where I often remind patients that soreness after exercise and fracture pain are not the same thing. Mild muscular fatigue can be acceptable. Sharp joint pain, increased swelling that lingers, or a sudden drop in motion is not.
Phase four return to real life and sport
The final phase is not about perfect clinic performance. It's about whether the arm works in the situations that matter to the person.
A return-to-function plan might include:
- Work tasks such as keyboarding, lifting files, tool use, or repeated gripping
- Home demands like cooking, child care, cleaning, or carrying groceries
- Recreational tasks including golf, tennis, climbing, yoga, or weight training
- Fall recovery strategies for older adults or those worried about reinjury
One-size-fits-all programs often fall short. The office worker needs endurance in low-load positions. The carpenter needs rotational strength and confidence under repeated force. The tennis player needs speed, deceleration control, and tolerance for impact through the hand and forearm.
For professionals, this phase is where the exam has to become specific. Don't stop at grip and goniometry. Look at task quality, movement strategy, apprehension, and whether the person can absorb load without guarding.
In outpatient practice, some patients use a clinic-based program, while others transition to an independent home plan after periodic reassessment. Services such as Highbar Physical Therapy are one example of outpatient PT for orthopedic and post-surgical recovery, where therapists tailor mobility, strengthening, and functional return work to the fracture pattern and the person's goals.
Recovery Timelines and Prevention Strategies
A patient gets the cast off, wiggles the fingers, and asks the question I hear every week. “So when will this feel normal again?” The useful answer is more specific than a date. Bone healing, joint mobility, strength, and trust in the arm recover on different timelines.
That difference matters because people often judge recovery by pain alone. A wrist can be much less painful and still be poorly prepared for turning a doorknob, catching a slip on the stairs, pushing up from a chair, or carrying a heavy pan with the forearm rotated. In radius injuries, especially those that affect alignment or joint mechanics, the lasting problems are often in rotation and load tolerance rather than simple soreness.
A practical timeline usually looks like this. Early healing is measured in weeks. Functional recovery often extends beyond that, particularly after a displaced fracture, surgery, prolonged immobilization, or a period of guarded use. Older adults, people with baseline stiffness, and patients returning to hand-intensive work often need more time because the problem is no longer just bone union. It is how well the whole arm accepts force again.
Alignment still shapes that outcome. As noted earlier, restoration of the radial bow is tied to better forearm function. In clinic terms, that means the bone has to heal in a shape that lets the radius rotate well around the ulna. If that relationship is off, pronation and supination can stay limited even when the fracture has technically healed.
This is why prevention starts before discharge from therapy. The goal is not merely avoiding another fracture. The goal is avoiding the predictable late deficits that follow under-treated stiffness, weakness, and deconditioning.
The prevention plan should match the mechanism of injury and the person's daily demands:
- After a fall: address balance, lower-body strength, home hazards, footwear, vision issues when relevant, and safe strategies for getting up from the floor
- After a sports injury: rebuild impact tolerance, timing, and technique before full return, especially in sports that require quick forearm rotation or weightbearing through the hand
- After a work-related injury: modify grip-heavy or awkward tasks, improve workstation or tool setup, and build enough endurance for repeated loading, not just a single test lift
- If bone quality is a concern: discuss nutrition, medication review, and bone-health screening with the physician, particularly when the fracture seems out of proportion to the force involved
Home symptom management has a role, but it should match the stage of recovery. Cold can help calm an irritated, swollen wrist after activity. Heat is often more useful before mobility work when stiffness is the main barrier. This guide on when to ice vs heat explains that choice in a way patients can use day to day.
Patients also ask about add-on recovery tools. If you're considering options such as pulsed electromagnetic field equipment, use that conversation the same way you would use a brace or a massage device. It may fit as an adjunct, but it does not replace fracture follow-up, progressive exercise, or graded return to loading.
The best prevention strategy is simple to say and harder to do. Restore motion early when cleared, rebuild strength in the ranges that matter, and train the arm for the exact tasks that caused trouble in real life. That is what lowers the chance of a “healed” radius becoming a chronically stiff, weak, or unreliable forearm.
Special Notes and How to Get Expert Help
Not every radius injury follows the same script. Two groups need especially careful decision-making: children and athletes.
Children are not just small adults
In pediatric cases, clinicians pay close attention to growth plates and remodeling potential. A child's bone can heal and adapt differently from an adult's, which can change both treatment decisions and how quickly function returns.
That said, growth plate injuries deserve respect. A fracture that looks straightforward to a parent may still need pediatric orthopedic follow-up because alignment and future growth matter together.
Athletes need more than basic clearance
An athlete may be pain-free in daily life and still be nowhere near ready for return to play. The demands are higher. The wrist and forearm must tolerate force, speed, repeated impact, and quick rotation under load.
For that reason, return decisions should consider more than comfort at rest. They should include sport-specific tasks, confidence, and whether the athlete can control the arm in positions that matter for performance.
When to get help sooner rather than later
A good recovery usually involves two tracks at once. The orthopedic team manages fracture healing and alignment. The physical therapist addresses motion, strength, swelling, scar mobility when relevant, and return to function.
Seek expert follow-up if you notice any of these issues:
- Persistent stiffness that isn't improving after immobilization ends
- Pain with rotation that limits daily tasks
- Swelling or hand dysfunction that lingers
- Weak grip or poor wrist control despite healing progress
- Fear of using the arm even after you've been medically cleared
Patients often think PT is only for people after surgery. That's not true. Many non-surgical radius fractures need guided rehab just as much, especially when rotation, grip, and wrist mechanics haven't come back cleanly.
If you're dealing with a radius bone injury, working with a physical therapist can help turn "the bone healed" into "the arm works again."
If your wrist or forearm still feels stiff, weak, or unreliable after a radius bone injury, a physical therapist can help you rebuild motion, strength, and confidence step by step. Highbar Physical Therapy provides outpatient rehab for orthopedic and post-surgical recovery, with treatment focused on restoring real-life function, not just checking that the fracture healed.