We've all seen it. A patient sits down to describe their problem, and when they go to stand up, they wince—a sharp, grabbing pain shoots through their hip. This classic complaint of hip pain when standing up from a sitting position is more than just a minor inconvenience; it’s a clinical puzzle waiting to be solved.
For physical therapists, this is one of the most common scenarios we encounter. It’s also one where our expertise can make a profound difference, turning a frustrating daily problem into a clear path toward confident movement. This guide breaks down a practical framework for decoding that pain and leading patients back to function.
Decoding the First Step: The Challenge of Sit-to-Stand Hip Pain

Getting up from a chair should be simple. But when that basic movement becomes painful, it signals a breakdown in the kinetic chain. As clinicians, our job is to pinpoint exactly what that is. Is the problem coming from inside the hip joint itself, or is an extra-articular structure the real source of the trouble?
This single moment is packed with diagnostic clues. It challenges us to think beyond a simple diagnosis and consider the entire picture—mechanics, anatomy, and the compensatory patterns the body has adopted. The leadership opportunity here isn't just identifying the source of pain, but understanding why this specific movement acts as the trigger.
Differentiating the Drivers of Pain
A strong evaluation begins with a clear differential. The pain a patient feels when they stand can stem from a few very different sources, and each one presents with its own tell-tale signs. Our goal is to connect the patient’s narrative to our anatomical knowledge and narrow down the likely culprits.
Here are the common causes we need to differentiate:
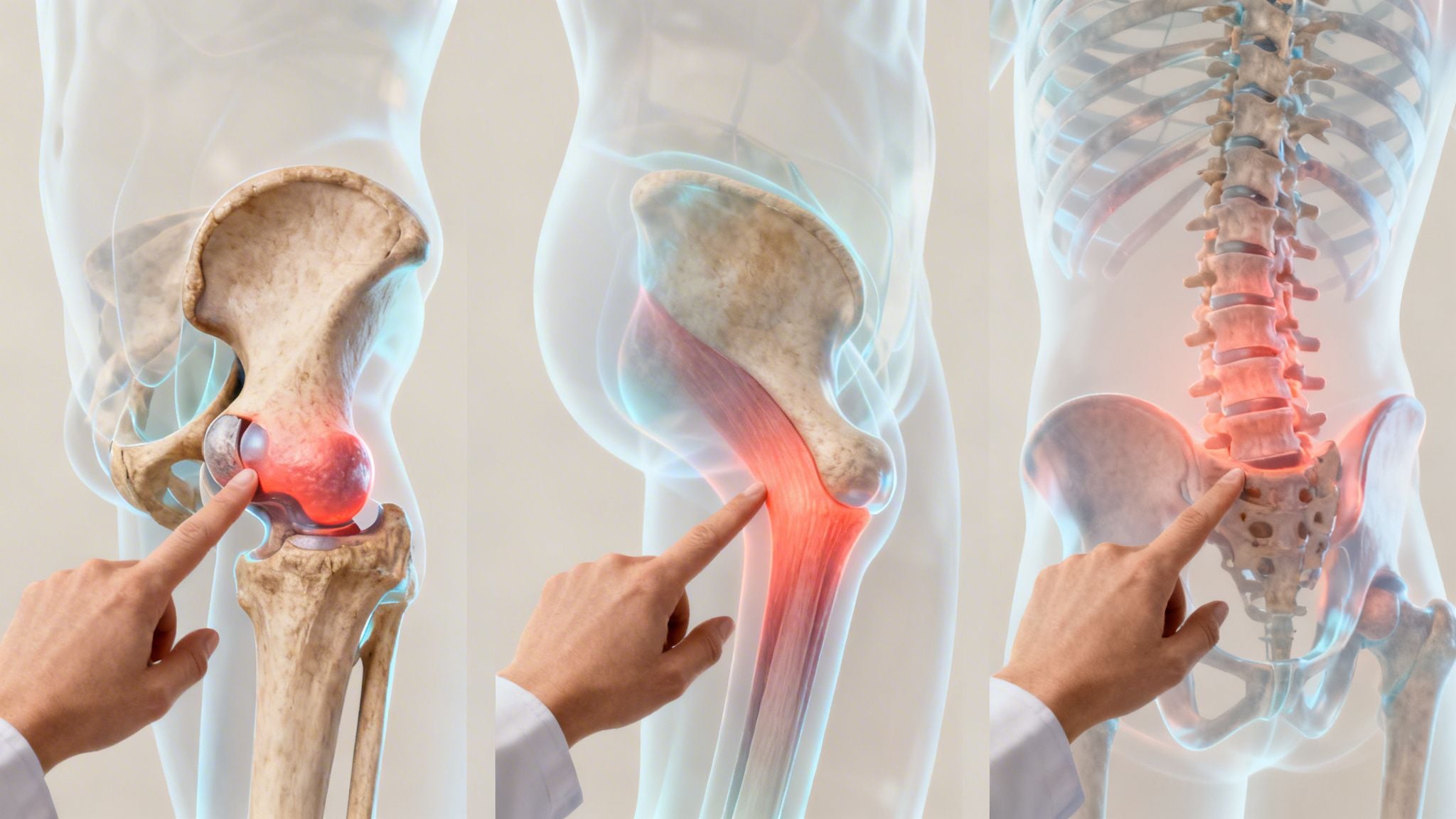
- Intra-articular Pathologies: These are problems inside the hip joint. Conditions like Femoroacetabular Impingement (FAI) or a labral tear often feel worse after sitting in deep flexion. As the patient stands, the hip moves into extension, which can cause a sharp, pinching sensation.
- Extra-articular Issues: This is pain from structures outside the joint. Gluteal tendinopathy is a prime example. Prolonged sitting can compress the tendons, and the powerful muscle contraction needed to stand up then stresses that irritated tissue.
- Referred Pain Patterns: We can never forget that pain isn’t always where the problem is. Pain originating in the lumbar spine or sacroiliac (SI) joint often refers to the hip and can be triggered by the load shift that occurs during standing.
- Muscular Imbalance: Often, the root cause is functional. Think tight, shortened hip flexors from prolonged sitting, paired with glutes that have become weak or inhibited. This creates a dysfunctional movement pattern where the body struggles to stand efficiently.
As clinicians, our true value lies in seeing the whole person, not just the symptom. Hip pain on standing is a story about movement, compensation, and an underlying problem we have the tools to interpret.
This guide provides a framework for doing just that. We'll move beyond textbook definitions to share practical, experience-driven insights. By sharpening your assessment skills, you can build confidence, deliver more effective treatment, and become the go-to expert your patients and colleagues trust.
Uncovering the Source: A Differential Diagnosis Framework
When a patient describes that sharp, stiff pain they get when standing up, our clinical minds should immediately start sifting through the possibilities. Moving from a vague complaint to a specific working diagnosis requires a systematic framework. It’s not just about listing potential causes, but truly understanding why each condition creates its unique brand of hip pain when standing up from a sitting position.
This is where we connect the patient’s story to the underlying anatomy. Think of yourself as a detective. The sit-to-stand movement is the scene of the crime, and each potential culprit leaves a distinct set of clues in the patient's narrative and our objective tests.
Intra-Articular vs. Extra-Articular: The First Big Question
The first fork in the road is deciding if the pain is coming from inside the joint (intra-articular) or outside of it (extra-articular). This single distinction shapes our entire examination and treatment plan.
Hip Osteoarthritis (OA) is a classic intra-articular cause. The story of morning stiffness or pain after sitting is often the "gelling phenomenon," where synovial fluid thickens during rest. When the patient stands, the joint surfaces, which may have worn-down cartilage, have to move without optimal lubrication. This creates that initial, intense pain that often eases after a few steps.
This isn't a rare problem. Frustration from hip pain with every sit-to-stand transition is something millions face, frequently tied to hip OA. Global research shows a dramatic surge, with a projection of 2,676,613 new cases by 2026 alone. You can find a deeper analysis in the full research on hip osteoarthritis trends.
On the other hand, gluteal tendinopathy, a common extra-articular issue, works on a totally different principle: compression. When someone sits, especially on a hard surface or with legs crossed, the gluteal tendons can get squeezed against the greater trochanter. The pain trigger isn't joint stiffness, but the sudden tensile load placed on that compressed and sensitized tendon during the powerful muscle contraction needed to stand.
A key clinical insight is to ask how the pain behaves in the first few steps. OA pain often feels like a stiff joint "warming up" and improving with movement, whereas tendinopathy pain can persist or worsen as the muscle continues to contract against resistance.
The Imposters: Lumbar Spine and SI Joint Referral
We’ve all seen it: the patient who presents with a "hip problem" that has nothing to do with the hip joint itself. The lumbar spine and sacroiliac (SI) joint are notorious for referring pain to the groin, buttock, and lateral hip, perfectly mimicking true hip pathology.
The sit-to-stand motion involves a major load shift and postural change for the entire lumbopelvic region. For a patient with underlying lumbar stenosis or disc pathology, moving from a flexed (sitting) to an extended (standing) spine can provoke their symptoms.
Likewise, an unstable or irritated SI joint can be aggravated by the asymmetrical forces required to shift weight and push up from a chair. The pain is often described as deep, achy, and harder to pinpoint than the sharp, localized pain of an intra-articular problem. This is exactly why a thorough lumbar and SI joint screen is non-negotiable in any hip evaluation. And when exploring less obvious sources, remember to consider conditions like pelvic floor dysfunction, where targeted interventions like pelvic floor massage therapy can be surprisingly effective.
Key Questions and Findings to Sharpen Your Diagnosis
To build your differential diagnosis efficiently, zero in on targeted questions and the hallmark findings for each condition.
-
For Hip Osteoarthritis (OA):
- Question: "Does the pain feel stiff and deep in the morning or after sitting, but then eases up a bit once you get moving?"
- Finding: Look for globally restricted range of motion, particularly in internal rotation and flexion, often with a firm, capsular end-feel.
-
For Gluteal Tendinopathy:
- Question: "Is the pain located on the outside of your hip? Does it hurt more when you lie on that side at night?"
- Finding: Point tenderness directly over the greater trochanter and reproduction of pain with a single-leg stance for 30 seconds are classic signs.
-
For Femoroacetabular Impingement (FAI):
- Question: "Do you get a sharp, pinching pain in the front of your hip or groin, especially when you sit in deep chairs or drive for a long time?"
- Finding: A positive FADIR test (flexion, adduction, internal rotation) that reproduces the patient's specific groin pain is a strong indicator.
-
For Lumbar/SI Referred Pain:
- Question: "Does the pain feel more like a dull ache that travels? Do you also have any back stiffness or pain?"
- Finding: Reproduction of hip symptoms with repeated lumbar extension or a positive SI joint provocation test (e.g., thigh thrust) points away from the hip joint itself.
The Hands-On Evaluation: A Systematic Assessment Approach

Once you have a working hypothesis, it's time for the hands-on evaluation. This is where we move from theory to confirmation, using a systematic physical exam to find the true source of their hip pain when standing up from a sitting position. An effective evaluation isn't a checklist of tests; it's a dynamic process of connecting each finding to the next.
The best place to start is with the painful movement itself. Before the patient even gets on the table, have them demonstrate the sit-to-stand motion. This simple, functional test is packed with diagnostic clues.
Observing the Sit-to-Stand: A Movement Analysis
Ask the patient to sit in a standard chair and then stand up at their usual pace. Watch them closely. You're looking for the subtle compensations their body makes to avoid pain. It’s not just about if it hurts, but how they move to manage that hurt.
Keep an eye out for these key indicators:
- Anterior Weight Shift: Do they lurch their trunk forward, using momentum instead of muscle? This often points to weak glutes and quads.
- Asymmetrical Loading: Does the patient push off heavily on their non-painful leg, effectively offloading the symptomatic side? This is a classic pain-avoidance strategy.
- Hand Assistance: Do they need to use their hands to push off the chair or their own thighs? This is a clear sign of significant weakness or pain-inhibition in the hip extensors.
- Visible Guarding or Pinching: Do you see them wince or instinctively grab the front of their hip as they rise? This "C-sign" is a strong clue for an intra-articular issue, like FAI or a labral tear.
These initial observations help you form a much sharper hypothesis, guiding your hands-on exam.
Essential Tests and Measures for the Hip
With your observational notes in mind, you can move to the examination table for a more structured assessment. Your goal is to systematically rule in or rule out the potential causes from your differential diagnosis.
1. Range of Motion (ROM) Assessment
Check both active and passive range of motion. Don't just measure the numbers; pay close attention to the end-feel and whether the movement reproduces their specific pain.
- Flexion and Internal Rotation: Limited and painful internal rotation, especially when paired with flexion, is a hallmark of intra-articular problems like OA or FAI. A firm, leathery end-feel suggests OA, while a hard, bony block could point to impingement.
- Extension: Pain on passive hip extension can signal tight or irritated hip flexors, a common culprit when standing up from a chair is painful.
2. Manual Muscle Testing (MMT)
Weakness is often both a cause and an effect of hip pain. Focus your MMT on the key muscles that stabilize the lumbopelvic-hip region.
- Gluteus Medius: Test this vital lateral hip stabilizer in a side-lying position. Weakness here is a primary finding in gluteal tendinopathy and contributes to pelvic drop during gait.
- Gluteus Maximus: As the main hip extensor, its strength is non-negotiable for a powerful sit-to-stand. Test it in prone with the knee bent to isolate it from the hamstrings.
- Iliopsoas: While often tight, the hip flexors can also be weak. Assessing strength provides a complete functional picture.
The real art of evaluation lies in synthesis. A single positive test is just a clue, but when you combine it with other findings, a clear diagnostic picture emerges.
Connecting the Dots with Special Tests
Special tests are designed to provoke specific tissues and are most powerful when interpreted within the context of your whole exam. For hip pain when standing, a few tests are particularly useful.
The FABER test (Flexion, Abduction, and External Rotation) is a fantastic screening tool. Anterior hip pain may suggest a hip flexor or joint issue, while posterior pain can point toward the SI joint.
The FADIR test (Flexion, Adduction, and Internal Rotation) is more specific. A positive test—one that reproduces that familiar anterior pinching pain—is highly suggestive of femoroacetabular impingement.
This is where you connect the dots. Let's say a patient showed an anterior pinch during the sit-to-stand observation. If they then have limited, painful internal rotation during ROM assessment and a positive FADIR test, you can be highly confident in a working diagnosis of FAI. This systematic approach transforms isolated findings into a compelling clinical narrative, setting you up for a targeted and effective treatment plan.
Recognizing Red Flags and When to Refer
As clinicians, one of our most critical skills is knowing the difference between a musculoskeletal problem we can manage and a symptom that requires referral. Hip pain when standing up is almost always within our scope of practice. However, clinical leadership demands we recognize those rare but crucial moments when the pain signals something more serious.
This isn’t just about risk management—it’s about ensuring patient safety and reinforcing our role as trusted primary care providers for musculoskeletal health. Knowing when to refer ensures every patient gets on the right care path.
Systemic Signs and Vascular Concerns
Some symptoms should immediately prompt you to think beyond a simple mechanical issue. These signs suggest the problem may not be musculoskeletal and could require urgent medical attention. Stay vigilant for:
- Constitutional Symptoms: Unexplained weight loss, persistent fever, night sweats, or malaise are classic red flags that can point to systemic issues like infection or malignancy.
- Vascular Claudication: If the patient describes hip or leg pain as a cramp that consistently appears after walking a certain distance and resolves with rest—not just on standing—your mind should shift to vascular causes. This is a very different pattern from the immediate pain of a sit-to-stand movement.
- History of Cancer: A patient with a past cancer diagnosis, especially prostate, breast, or lung cancer, who presents with new, unprovoked hip pain needs an immediate workup to rule out metastatic disease.
Neurological Deficits and Trauma History
Progressive neurological changes are another clear signal to refer. While we often treat minor nerve irritation, rapidly worsening deficits are a different matter. Be on the lookout for progressive muscle weakness, changes in reflexes, or any hint of saddle anesthesia or bowel/bladder dysfunction, which require an emergency referral.
A patient’s history of trauma is a critical piece of the puzzle. A significant fall, especially in an older adult or someone with osteoporosis, should create a high index of suspicion for a fracture, even without obvious deformity. If a patient is unable to bear weight after a fall, referral is mandatory.
Hip pain when rising from a chair can sometimes be a precursor to more significant events. The underlying issues can contribute to hip fractures, which hit 14.2 million cases globally in 2019—a staggering 92.7% increase since 1990. Recognizing this potential is vital; you can explore more about the global burden of hip fractures to grasp the scale. For patients whose pain is clearly tied to joint deterioration, our guide to managing arthritis and osteoarthritis offers deeper insight into our treatment approach.
Crafting a Plan: A Phased Approach to Treatment

Once we've established a working diagnosis, we shift to action. A great treatment plan is more than a list of exercises; it's a phased roadmap designed to first calm symptoms, then restore function, and finally build resilience.
Our strategy is to de-escalate the irritated tissues and then progressively re-introduce mobility, strength, and correct movement patterns. We’re not just chasing pain; we’re fixing the root problems so patients can move with confidence long after discharge.
Phase 1: Pain and Inflammation Control
Before we can rebuild, we have to put out the fire. When a patient is highly irritable, our first job is to reduce pain and inflammation. This phase relies heavily on manual therapy and patient education on activity modification.
Manual therapy can provide immediate relief. For a patient with hip OA, gentle joint mobilizations can improve synovial fluid movement and ease that "stuck" feeling. For gluteal tendinopathy, careful soft tissue work around the hip can release surrounding muscle tension while avoiding direct pressure on the sensitized tendon.
We also coach patients on how to stop provoking their symptoms. Smart modifications might include:
- Adjusting chair height: Ensuring the hips are level with or slightly above the knees reduces stressful deep flexion.
- Using a cushion: A simple wedge cushion can tilt the pelvis forward, offloading compressed gluteal tendons.
- Taking movement breaks: Getting up to walk for a few minutes every hour is a game-changer for preventing stiffness.
Phase 2: Mobility and Flexibility Restoration
Once the acute pain is under control, we can work on restoring full range of motion. The mobility drills we choose are specific to the diagnosis—this is not a one-size-fits-all approach.
- For Hip Osteoarthritis: We focus on restoring capsular mobility. Gentle, hands-on rotational mobilizations followed by self-stretches like the figure-4 can help reclaim lost rotation.
- For Tight Hip Flexors: The go-to is the half-kneeling hip flexor stretch. The key is teaching the patient to posteriorly tilt their pelvis before leaning forward to isolate the stretch effectively.
- For Referred Pain from the Lumbar/SI Region: Nerve glides (neurodynamics) can be incredibly effective. Techniques like sciatic nerve sliders help desensitize the nerve and relieve deep buttock and thigh pain.
Think of this phase as giving the joint and surrounding tissues the freedom they need to move correctly. If we skip this step, any strengthening we do later will just reinforce compensatory movement patterns.
Phase 3: Strength and Motor Control
This is where we build a lasting solution. We retrain the muscles to properly support the hip and control the sit-to-stand motion. The focus is on progressively loading the glutes, core, and hip extensors.
We always start with activation exercises before progressing to more functional strength work. For example, a patient with gluteal tendinopathy might begin with isometric hip abduction against a wall to activate the muscle and provide an analgesic effect without compressing the tendon. From there, we might progress to standing hip abduction with a resistance band, and eventually to functional movements like lateral band walks.
Here are a few real-world examples:
- FAI Patient: We use controlled box squats to reteach the hip hinge. We cue them to "send the hips back" while keeping the spine neutral, training them to load their glutes and hamstrings without pinching the anterior hip.
- Gluteal Tendinopathy Patient: We start with bridges, cueing them to feel it in their glutes, not their hamstrings. We then progress to a single-leg bridge to challenge pelvic stability.
- General Deconditioning: We use the sit-to-stand motion as the exercise itself. By controlling the depth, speed, and using external load, we build both strength and motor control in the exact pattern that was painful.
By moving step-by-step from pain relief to mobility and finally to strength, we’re not just helping patients feel better in the short term. We’re empowering them with the physical capacity and confidence to move freely again.
Leading Through Education: Empowering Patient Self-Efficacy
Great clinicians don’t just treat; they empower. Beyond our manual techniques and exercise prescriptions, our most lasting impact comes from helping patients understand the "why" behind their pain. This is never more true than with a complaint as frustrating as hip pain when standing up from a sitting position. When we shift the focus from just what to do to why it works, we build patient confidence and self-efficacy.
This is the crucial final step in our care plan. It’s about creating change that sticks, ensuring the patient understands their body well enough to manage flare-ups long after their formal sessions with us are over.
Translating Clinical Knowledge into Patient Understanding
Explaining complex anatomy in simple, memorable terms is a skill that builds immense trust. Instead of just saying "your hip flexors are tight," we can give them an analogy they’ll actually remember.
"Think of your hip flexors like bungee cords. When you sit all day, those cords are held in a short, tight position. Standing up suddenly is like yanking on them—they resist and send a 'threat' signal to your brain, which you feel as pain. Our goal is to teach those bungee cords how to lengthen properly again."
This simple picture completely reframes their pain. Suddenly, the exercises we prescribe aren’t a chore; they’re the solution. When a patient understands that a half-kneeling stretch is "letting the bungee cord relax," they are far more likely to adhere to their program.
Empowering Patients with Proactive Strategies
Our role as educators must extend into the patient's daily environment. We need to arm them with practical strategies to navigate their world without constant symptom provocation. This is where we share our expertise on ergonomics and habit formation.
Here are a few key self-management strategies to teach:
- The Ergonomic Audit: Show them how to set up their workstation. This means adjusting chair height so their hips are slightly above their knees and using a small lumbar roll to maintain a neutral pelvic position.
- The Power of Movement Breaks: Remind them that the body is made to move. Suggest setting a timer to get up and walk around for 2-3 minutes every hour. This prevents that stiff, "gel-like" feeling from setting in.
- Flare-Up First Aid: Give them a simple, two-step plan for when they overdo it. This could be a sequence of gentle, pain-free mobility drills followed by applying heat to ease muscle tension.
By providing this framework, we turn patients into active participants in their recovery. We're not just offering a temporary fix; we're giving them the tools for long-term health. For more detailed guidance, you can point them to resources on arthritis management or discuss ideas for improving workplace ergonomics. It's all about leading them to a place where they feel in control of their bodies and confident in their movement.
Frequently Asked Questions From Our Clinicians
As leaders and mentors in physical therapy, we get a lot of nuanced questions that don't have simple textbook answers. When it comes to something as common as hip pain when standing up from a sitting position, our colleagues are always looking for practical advice rooted in real clinical experience. Here are a few common questions that come up in our clinics.
How Do You Differentiate Lumbar Referred Pain from True Hip Pathology?
This is a classic clinical challenge. The best place to start is with a thorough lumbar screen. Have the patient perform repeated lumbar movements and watch closely to see if their hip symptoms centralize or peripheralize. That simple test often gives you a clear answer.
A positive straight leg raise (SLR) or slump test can also point you toward neural tension as a contributor. If the patient describes the pain as vague or diffuse—and you can't reliably reproduce it with direct palpation or specific hip movements like the FADIR test—your suspicion should turn toward the spine.
What Are the Best First-Line Exercises for Suspected Gluteal Tendinopathy?
With gluteal tendinopathy, the first job is to calm things down without provoking the tendon. You want to load the tendon without compressing it, so the best place to begin is with isometric loading exercises.
An isometric hip abduction against a wall is a simple, effective starting point. Have your patient hold the contraction for 30–45 seconds at an intensity that feels moderate but doesn't stir up their pain. It’s critical to avoid positions that compress the tendon, like deep side-lying clamshells or aggressive IT band stretching, especially in the early, irritable stage.
When Should a Clinician Recommend Imaging for This Type of Hip Pain?
Imaging should almost never be the first step. The time to recommend it is if you see red flags that suggest something more serious, like a fracture or avascular necrosis. This is especially true if the patient has a history of major trauma, long-term corticosteroid use, or constitutional symptoms.
It may also be time for imaging if a patient with a suspected FAI or labral tear fails to progress after a solid 6–8 week trial of evidence-based conservative PT. In those cases, collaborating with the referring physician to suggest an X-ray or MRI can help confirm the diagnosis and guide next steps.
What Is a Key Cue to Improve Sit-to-Stand Mechanics?
One of the most powerful cues I use is “lead with your chest, not your head.” This simple phrase encourages a proper hip hinge and discourages that excessive forward trunk lean that puts so much stress on the anterior hip. It naturally gets the patient to load through their hips and legs instead of just using momentum.
Another great one is to tell the patient to “push the ground away” as they stand up. This cue helps them activate their glutes and quads, leading to a much stronger and more stable movement. Practicing this with controlled box squats is a fantastic way to retrain that motor pattern. For patients' home or work environments, it can also be useful to discuss ergonomic seating and explain how a saddle chair can help relieve hip pain.
